Shoulder Joint examination Overview
500 likes | 959 Vues
Shoulder Joint examination Overview. Introduction Presentation Examination Anatomy Investigations Injections Key points. A J Chakrabarti FRCS(Orth). Introduction. Shoulder pain is very common Can be Recalcitrant Many get better spontaneously without treatment

Shoulder Joint examination Overview
E N D
Presentation Transcript
Shoulder Joint examinationOverview Introduction Presentation Examination Anatomy Investigations Injections Key points A J Chakrabarti FRCS(Orth)
Introduction • Shoulder pain is very common • Can be Recalcitrant • Many get better spontaneously without treatment • Costly
Introduction Rheumatology 2006;45:215–221 • Prevalence • Overall 7% • 26% in elderly
Shoulder Pain in Adults Secondary Care Rxs 20% Manages 80% Primary Care Community 50-80% Do not present
Not getting better spontaneously • What is the actual diagnosis? • Are there specific considerations for this particular patient? • When should I refer?
Basic steps History Examination Clinical tests Investigations XR/US Shoulder examination • What is the diagnosis ? • Don’t be too hasty in simply diagnosing “Frozen shoulder”
Lifestyle Occupation Handedness Sports/Hobbies Patient factors of importance • PMH / PSH • DH • Expectations • Previous treatments
Pain Stiffness Instability Weakness/ Functional loss Shoulder Complaints • Swelling • Deformity • Electrical disturbance/ Vascular disturbance
Pain Shoulder Complaints • That keeps patient awake at night
Pain Shoulder Complaints • Keeps partner / spouse up! Groan
Onset Injury Duration Site Severity Nature Periodicity Timing Shoulder ComplaintPain • Night pain • Exacerbating • Relieving factors • Treatments tried • Tablets • Response to Rxs
Injury Shoulder ComplaintPain • Nature • Bleeding/ Bruising • Snap. Crack • “General Feel” • Position of arm • Pre-existing state
Radiating to forearm/hand infrequent Radiating to neck Does not arise form intrinsic shoulder problems (except ACJ- to base of neck) Site ofPain
Shoulder ComplaintPain • Open Palm v Finger sign • Deltoid sited pain • Subacromial space / Rotator cuff. GHJ • Superiorly sited pain • Acromioclavicular joint
Shoulder Instability • Traumatic • Atraumatic • GLL • Muscle patterning disorder • History of fits • Event • Ease • Frequency • Subtle instabilities • Pain • Dead arm
Shoulder Weakness • Pain causes weakness • Weakness of muscles –neural, musculotendinous or other mechanical • Patients exact meaning • Association with any pain.
Remember that pain experienced in the shoulder can arise from outside the shoulder Painful Shoulder
Shoulder Complaints • Neck • Brachial plexus pain • Viscera. Intrathoracic/ subphrenic • Chronic regional pain syndromes
Neck Brachial plexus pain Viscera. Intrathoracic/ subphrenic Chronic regional pain syndromes Shoulder Complaints
Shoulder examination • Multiple techniques • No best single way! • Compare sides
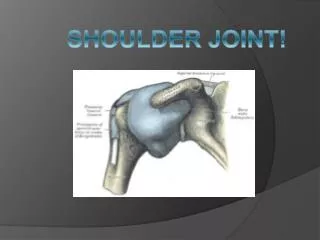
Glenohumeral joint Acromioclavicular joint Sternoclavicular joint Subacromial space Rotator Cuff Scapulothoracic articulation Assessing a ShoulderAnatomic sites Three True Joints Three areas Think anatomically !
4 muscles with their tendons acting as a functional unit to maintain the humeral head centered on the glenoid The Rotator cuff
Clinical Examination • Look • Feel • Move • Stand • Sit • Lie
Clinical Examination • Inspection • Localising Tenderness • Neck Examination CxSp • Neuro exam • Functional assess • Elevation • Impingement • ER • IR • Abduction RPA • Cuff testing 3 pt • Biceps
Minimum 10 point Clinical Examination • Inspection • Localising Tenderness • Neck Examination CxSp • Neuro exam • Functional assess • Elevation • Impingement • ER • IR • Abduction RPA • Cuff testing 3 pt • Biceps
Empty can Impingement • PositiveComparative increased painNo pain But slowerBlock
The Hallmarks of common diseases • Cx stiffness/ pain: Cervical spondylosis / Cx disc prolapse • Elevation restriction: RCT lifting with good arm • Impingement sign: Bursal/cuff disease or ACJ impingement • Restrictions of Global GHJ motion: Capsular contracture of Frozen shoulder or OA GHJ • Loss of resisted muscle power: RCT or pain inhibition • Painful resisted cuff activity: RCT/ impingement • LHB signs: Biceps tendinopathy
10 point examination Clinical Judgement Neck Shoulder ACJ BURSA CUFF BICEPS CAPSULE AND JOINT SURFACE
Shoulder Scores of function • Oxford Shoulder Score 48 • 12 Questions – all relate to shoulder in last 4 wks • 0-4 per question. Max score 48/48 = Gd shoulder • Worst,Dressing,Car,Knife,Shopping,Tray • Brush,Usual,Robes,Axilla,Housewk,Night
Does it need an XR? Yes: If referring for surgical opinion Yes: If you need it to corroborate your diagnosis Yes: If possibility of calcific disease Yes: If need to exclude arthrosis (The arthrosis of ACJ The arthrosis of the GHJ) Yes: If concerned re: malignant disease
AP 30° Caudal Axillary Lateral Stryker Notch view for GHJ instability Clavicular views for ACJ instability What XR’s do I find valuable?
Ultrasound examination Examines the rotator cuff Supraspinatus Infraspinatus Subscapularis Teres Minor Long Head Biceps Bursa / Impingement
Ultrasound examination DO NOT REQUEST IN PREFERENCE TO PLAIN XR FILM
MRI? Access to the films is the most important The reports may be misleading. The MRI has a picture that both clinician and patient can understand Most useful when: ACJ impingement a possibility Other pathologies /multiple pathologies are expected Limited use without contrast: calcific disease/ instability
Treatments In all cases Conservative. Analgesia Physiotherapy: Pendular exercises Theraband exercises Eccentric Deltoid exercises “eccentric means lengthening during loading” Steroid injections Other injections / other treatments
Treatments Theraband exercises
Steroid Injections Prep the skin and draw up solution with separate needle to one used to inject. Portal: Soft spot – Below Postero-lateral corner Aim for Anterior acromion for bursal injection Aim for Coracoid process for GHJ injection Superior Summit for ACJ
Cures for shoulder diseases? Arthritis ACJ: Excision arthroplasty Arthritis GHJ: Total shoulder replacement/ Hemi Rotator Cuff Arthropathy: Reverse polarity prosthesis Acute Rotator Cuff Tears: RCR Impingement with/without Tears: ASAD Instabilities: Various stabilizations
Conditions that may not be cured Chronic Calcific Disease: Massive Cuff Tears: Degenerative RCTears without arthritis: Poor vascularity Secondary fatty infiltration and neural change to muscle/tendon unit Patients unfit for surgery: Conservative management: Steroid injections/ Eccentric Deltoid Training/ Suprascapular Nerve Blocks
Prognosis in shoulder conditions is largely determined by the condition of the rotator cuff andThe outcome following surgery in most cases largely determined by the condition of the rotator cuff