Download
1 / 24
350 likes | 2.12k Vues
Spore Forming and Non-Spore Forming Gram-positive Bacilli 10 th January 2007. SBM 2044 Medical Microbiology Second year UG of BBiomedic Sc. Spores. Why do bacteria produce spores? Survival Classification

E N D
Spore Forming and Non-Spore Forming Gram-positive Bacilli10th January 2007 SBM 2044 Medical Microbiology Second year UG of BBiomedic Sc
Spores • Why do bacteria produce spores? • Survival • Classification • Definition = a resting cell, highly resistant to dessication, heat, and chemical agents; when returned to favourable conditions bacteria re-activated, the spores germinate to produce single vegetative cells.
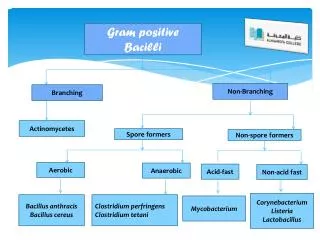
Bacillus • Aerobic, G+ rods in chains, spores are located in center of the non-motile bacilli • Found in soil, water, air and vegetation • Spores are viable for decades. • B. cereus – produce enterotoxin and cause food poisoning. • B. anthracis – infection in human through injured skin (cutaneous anthrax), mucous membranes (GI anthrax), or inhalation of spores into lung.
Bacillus • Spores germinate in the tissue of entry, and growth of vegetative organisms result in formation of a gelatinous oedema and congestion. • Spread via lymphatics to bloodstream and multiply freely in blood and tissues. • Capsulated, poly-D-glutamic acid capsule is antiphagocytic
Bacillus • Anthrax toxin is made up of three proteins: • Protective antigen (PA), oedema factor (EF) and lethal factor (LF). • Treatment: ciprofloxacin, penicillin G along with gentamicin and streptomycin. Vaccine with live spores and a toxoid used to protect livestock in endemic areas.
Clostridium • Anaerobic, G+, motile rods, typical tennis racquet morphology is created by terminal spores that swell the sporangium • Clostridial diseases from wounds inc tetanus (NM disease) and gas gangrene (soft tissue infection that damages muscle) • Found in soil, animal faeces. • Spores is placed centrally, subterminally or terminally; most species are motile with flagella.
Clostridium • Many form colonies with a zone of haemolysis on blood agar. C perfringens typically produce multiple zones of haemolysis around colonies.
Clostridium botulinum • C botulinum causes botulism, from eating poorly preserved food (canned). • Spores are resistant to 100°C for many hours, diminished at acid pH or high salt. • C botulinum is distinguished by antigenic type of toxin • Toxin - 7 antigenic varieties (A →G). A, B, E (F) mainly harmful to human. • Botulinum toxin is absorbed from gut and binds to receptors of presynaptic nervous system and cranial nerves.
Clostridium • Toxin acts by blocking release of acetylcholine at synapses and neuromuscular junctions → flacid paralysis. • Symptoms such as visual disturbances, inability to swallow, speech problem; seldom with no apparent GI symptoms; no fever. • ‘floppy baby’ = infant botulism. C botulinum spores ingested from babies’ food. Present with weak sucking response, loss of tone and respiratory complications.
Clostridium • Treatment – antitoxins raised in horses. • Trivalent (A, B, E) antitoxin must be promptly administered intravenously with precautions; plus adequate ventilations. • Treatment to control the microbe’s growth and toxin production. • Clostridium tetani cause tetanus or lockjaw.
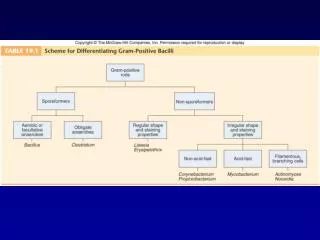
Non-Spore Forming Bacteria • Generally, members of normal flora of skin and mucous membranes of humans.
Corynebacterium diphtheriae • Infects nasopharynx or skin • Mostly grow aerobically, non-motile • Irregular swellings/clubbed-shaped; granules within rod stained with aniline dyes.
Corynebacterium diphtheriae • Blood agar+potassium tellurite, tellurite is reduced intracellularly which gives the black/gray coloured appearance.
A B Inhibits polypeptide chain elongation, by inactivating EF-2 (with NAD) This abrupt arrest of protein synthesis results in necrotizing and neurotoxic effects of Dt. Transporting A into cell Corynebacterium diphtheriae • In respiratory wounds, skin of infected person; spread by droplets or contact to susceptible individuals • Diphtheria toxin (Dt) is a single polypeptide chain, 62000 Mw; a heat-labile. • Dt cleaved into two polypeptide fragments following mild-digestion with trypsin and reduction under denaturing conditions.
Corynebacterium diphtheriae • Pathogenesis is based upon: (1) the ability of a given strain of C diphtheriae to colonize in the nasopharyngeal cavity and/or on the skin, and (2) its ability to produce diphtheria toxin. • Pathology: Dt absorbed into mucous membranes, causing destruction of epith and superficial inflammatory response. Necrotic epith embedded in exuding fibrin+RBC+WBC= grayish “pseudomembrane” • Disease is principally result of the action of toxin formed rather than invasion by the organism
Corynebacterium diphtheriae • Vaccination confers protection against disease by production of antibodies to the diphtheria toxin. The vaccine is produced from purified inactivated toxin from a strain of C. diphtheriae. • Diphtheriae antitoxin (DTP) administered to infants, and followed by boosters. • Treatment rapid suppression of toxin-producing bacteria by antimicrobial drugs at the earliest diagnosis of diphtheria.
Listeria monocytogenes • Small/Short, G+,peritrichous flagella, rod. Grow on Mueller-Hinton agar (better in sheep blood-small zone of haemolysis); facultative anaerobe, motile at room temp, catalase + • Listeriosis results from ingestion of contaminated food such as cheese and vegie; primarily affects pregnant women, newborns, those with weakened immune system. • Able to multiply at low temp, hence accumulate in contami- nated food stored in refrigerator.
Steps in the invasion of cells and intracellular spread by L. monocytogenes. • The bacterium apparently invades via the intestinal mucosa. It is thought to attach to intestinal cells by means of D-galactose residues on the bacterial surface which adhere to D-galactose receptors on susceptible intestinal cells The bacterium is taken up by induced phagocytosis, which is thought to be mediated by a membrane associated protein called internalin. Once ingested the bacterium produces listeriolysin to escape from the phagosome. The bacterium then multiplies rapidly in the cytoplasm and moves through the cytoplasm to invade adjacent cells by polymerizing actin to form long tails.
Actinomycetes • Form chains or filaments, facultative anaerobes (+CO2) • Actinomycosis is a chronic suppurative and granulomatous infection that produces pyogenic lesions with interconnecting sinus tracts that contain granules. Most cases due to A israelii, A naeslundii. • Commonly affecting cervicofacial, thoracic and abdominal actinomycosis.
References • Brooks’ Jawetz Medical Microbiology http://textbookofbacteriology.net/ • http://www.gsbs.utmb.edu/microbook/ • Puan Intan Azura Shahdan • Room F2/A/2/73