BIO 169 THE URINARY SYSTEM CHAPTER 26
830 likes | 1.29k Vues
BIO 169 THE URINARY SYSTEM CHAPTER 26. created by Dr. C. Morgan. TOPICS. Introduction and Organization Kidney Structure and Blood Supply Renal Physiology Urine Transport, Storage, and Elimination Aging and the Urinary System. Resource: IPCD Urinary System.

BIO 169 THE URINARY SYSTEM CHAPTER 26
E N D
Presentation Transcript
BIO 169 THE URINARY SYSTEM CHAPTER 26 created by Dr. C. Morgan
TOPICS Introduction and Organization Kidney Structure and Blood Supply Renal Physiology Urine Transport, Storage, and Elimination Aging and the Urinary System Resource: IPCD Urinary System
Introduction and Organization Objectives Discuss the role of the urinary system. List the functions of the urinary system List the organs of the urinary system. Briefly characterize the nature of urine.
Introduction and Organization After your blood has completed tissue exchange, it contains quantities of waste products, increased CO2, and perhaps imbalances of electrolytes. Your lungs eliminate the excess CO2. Since the blood is reused, somehow it must be cleansed of the other wastes and its fluid volume and electrolytes adjusted on a continual basis. The role of the kidneys is to perform these tasks. These activities are closely regulated and cellular life of all tissues is closely integrated with the urinary system via the blood.
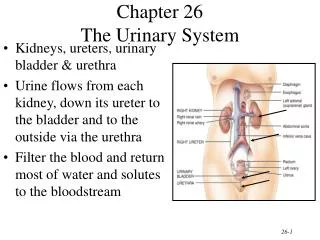
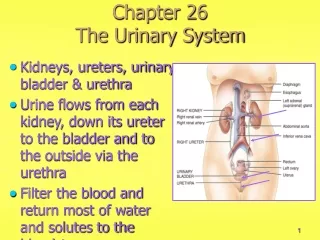
Introduction and Organization (cont) The functions of the urinary system are: *to regulate fluid volume and blood pressure *to regulate plasma ion concentrations *assist in the homeostasis of blood pH *to conserve nutrient molecules, especially glucose and amino acids *to rid the body of organic waste products *help the liver to detoxify poisons The organs are the kidneys, ureters, urinary bladder and urethra. Urine is a filtrate of the blood made by the kidneys, stored in the bladder, and eliminated from the body via the urethra.
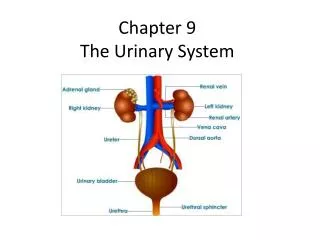
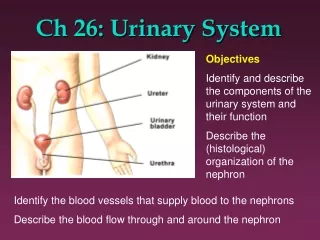
Introduction and Organization (cont) Urinary System Organs Fig. 1
TOPICS Introduction and Organization Kidney Structure and Blood Supply Renal Physiology Urine Transport, Storage, and Elimination Aging and the Urinary System
Kidney Structure and Blood Supply Objectives Examine the gross anatomy of the kidneys. Study the sectional anatomy of the kidneys. Describe the blood supply to the kidneys. Discuss the innervation of the kidneys. Describe the structure of the nephron and collecting system.
Kidney Structure and Blood Supply (cont) retroperitoneal Fig. 2 a
Kidney Structure and Blood Supply T12 – L3 level Fig. 2 b
Kidney Structure and Blood Supply (cont) Sectional Anatomy Fig. 4 a
Kidney Structure and Blood Supply (cont) Renal Blood Flow Fig. 5 b Fig. 5 a
Kidney Structure and Blood Supply (cont) Renal Blood Flow 20 – 25% of the cardiac output flows through the kidneys (1200 ml / minute) Fig. 5 c,d
Kidney Structure and Blood Supply (cont) Innervation: Renal nerves, mostly postganglionic sympathetic fibers from the mesenteric ganglion, branch to follow the tributaries of the renal arteries. Sympathetic fibers reach each nephron. Sympathetic output *changes the blood flow and pressure at the nephron *and stimulates the release of renin (RAA response)
Kidney Structure and Blood Supply (cont) The nephron is the functional unit of the kidney. There are about 1.25 million nephrons / kidney residing in the outer medulla and cortex. About 85% of all nephrons are situated in the kidney cortex so are called cortical nephrons. 15% of the nephrons are called juxtamedullary nephrons because they have long loops of Henle that project into the medulla. The peritubular capillaries that surround these nephrons are continuous with the vasa recta, a parallel capillary loop that is adjacent to the loop of Henle. The juxtamedullary nephrons give the kidneys the ability to produce a very concentrated urine.
Kidney Structure and Blood Supply (cont) Two types of nephrons Fig. 7 a
Kidney Structure and Blood Supply (cont) Peritubular capillaries surrounding a cortical nephron Materials are exchanged between the peritubular capillaries and the surrounding interstitium. Fig. 7 b
Kidney Structure and Blood Supply (cont) Peritubular capillaries and vasa recta surrounding a juxtamedullary nephron Fig. 7 c
Kidney Structure and Blood Supply (cont) The Nephron TABLE 1 Fig. 6
Kidney Structure and Blood Supply (cont) A filtrate of the blood is formed in the renal corpuscle. The renal corpuscle consists of Bowman’s capsule containing a knot of capillaries called the glomerulus. Extending from the capsule is a long renal tubule which is divided into regions, each characterized by cells with unique structural features. The renal tubule empties into a collecting duct which is continuous with a collecting system. Once the filtrate reaches the papillary duct of the collecting system it will undergo no more changes so may be called urine.
Kidney Structure and Blood Supply (cont) The nephron and collecting ducts engage in three activities: filtration, reabsorption, and secretion. Filtration of the blood occurs across the walls of the glomerular capillaries to form a filtrate that passes through the tubules of the nephron and collecting duct. As the filtrate passes through the tubules, it is modified. Reabsorption is the process of moving the materials to be kept back to the blood vascular system. Secretion is moving some substances from the interstitial space into the filtrate so it is eliminated in urine. Special characteristics of the cells along the length of the nephron accomplish these tasks using the transport mechanisms familiar to you (diffusion, facilitated diffusion, co and active transport).
Kidney Structure and Blood Supply (cont) Renal corpuscle Filtration membrane 22 Fig. 8 b
Kidney Structure and Blood Supply (cont) Podocytes are specialized epithelial cells that cover the surface of the glomerular capillaries with adjacent processes called pedicles. The podocytes are continuous with the epithelial cells that form the capsular wall. The capillaries are very permeable because they have pores (fenestrations). Filtrate flow: fenestrations capillary lamina densa slits between pedicles capsular space. filtration membrane Fig. 8 d 23
Kidney Structure and Blood Supply (cont) The filtration membrane will not let red blood cells and large proteins through so they are retained in the blood as important osmotic pressure components. Crossing the membrane to become filtrate components are water, electrolytes, glucose, amino acids, vitamins, metabolic waste products, fatty acids, and additional miscellaneous solutes. The solutes and water that are needed by the body must be recovered by reabsorption as the filtrate passes along the tubules and collecting system. Glomerulonephritis is an inflammatory condition caused by an abundance of Ag/Ab complexes that clog the filtration membrane thereby slowing filtration.
Kidney Structure and Blood Supply (cont) The proximal convoluted tubule is the first segment of the nephron. Glucose, amino acids, some proteins, and ions are transported from the filtrate into the interstitial space outside the PCT with water following by osmosis. Some secretion of H+ (ammonium, creatinine, drugs, and toxins) also occurs in the PCT. Microvilli increase the surface area of cuboidal cells making up the PCT. 60–70% of the filtrate volume is reabsorbed in the PCT.
Kidney Structure and Blood Supply (cont) The PCT descends toward the medulla to become the first “leg” of the loop of Henle. There are thick and thin segments in the loop of Henle. The thick segments consist of cuboidal cells. The thin segments consist of squamous cells. The ascending limb thick segment cells pump Na+ and Cl¯ out into the interstitium. The interstitium of the medullary region contains a progressively greater concentration of solutes toward the renal pelvis. Water moves out of the permeable thin segments due to the osmotically concentrated medullary interstitium.
Kidney Structure and Blood Supply (cont) The cells of the thick segment of the ascending limb of the loop of Henle are impermeable to water and solutes but as Na+ and Cl¯ are actively transported into the interstitium the filtrate becomes progressively less concentrated than the blood. The thick segment of the loop of Henle makes a sharp bend near the renal corpuscle to become the distal convoluted tubule (DCT). DCT cells do not have microvilli. The DCT is the site of active secretion of H+ ions, acids, or other molecules along with additional selective reabsorption of Na+ and Ca2+ from the remaining filtrate. Water may also be selectively reabsorbed in the DCT.
Kidney Structure and Blood Supply (cont) At the junction with the ascending limb of the loop of Henle, a group of the DCT cells, the maculadensa cells, are special because they contact some modified smooth muscle cells in the wall of the afferent arteriole that delivers blood to the renal corpuscle. The smooth muscle cells are the juxtaglomerular cells which secrete the enzyme renin (RAA cascade of events for blood pressure control) and erythropoietin. Together these cells form the juxtaglomerular apparatus (JGA).
Kidney Structure and Blood Supply (cont) the JGA Fig. 8 b
Kidney Structure and Blood Supply (cont) As the filtrate again passes toward the renal pelvis through the collecting ducts and papillary duct, its concentration is adjusted by hormonally regulating water, Na+, and bicarbonate ion reabsorption as well as some final secretion. The collecting system path: Collecting ducts papillary ducts minor calyx major calyx renal pelvis. Cells of the collecting system are columnar epithelium.
Kidney Structure and Blood Supply (cont) Review Reabsorbed materials pass from tubular filtrate into the interstitial space then into the capillaries. TABLE 1 Secreted materials pass from capillaries into the interstitial space and then into the filtrate.
TOPICS Introduction and Organization Kidney Structure and Blood Supply Renal Physiology Urine Transport, Storage, and Elimination Aging and the Urinary System
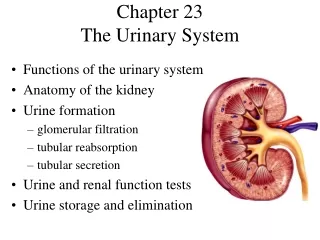
Renal Physiology Objectives Discuss the role of the kidneys in excretion of wastes. Describe the fluid dynamics affecting filtration. Discuss the regulation of renal function by autoregulation and neural mechanisms. Describe the events of reabsorption. Describe the events of secretion. Discuss countercurrent exchange. Discuss hormonal control of kidney function. Describe the composition of normal urine.
Renal Physiology The kidneys function to regulate the volume and composition of the blood. Cellular metabolism generates a number of organic waste products that end up as dissolved solutes in the blood which must be removed from the body. Urea, generated from the breakdown of amino acids, represents most of the organic waste (21 g / day). Creatinine is generated in muscle tissue as creatine phosphate is broken down (1.8 g / day). Uric acid is generated by the breakdown of nucleic acids and recycling of RNA (480 mg / day). The kidneys can spare water loss by excreting a urine that is 4 to 5 times more concentrated than normal body fluids.
Renal Physiology (cont) Although urine is a filtrate of the blood, its composition is very different from other body fluids (see TABLE 2). Kidney function embraces the three processes, filtration, reabsorption, and secretion (see TABLE 3). Filtration: The blood pressure is the driving force for filtration at the glomerulus, the only place filtration occurs. Because there are forces that oppose filtration, the critical factor is the net filtration pressure (NFP). The diameter of the afferent and efferent arterioles may be controlled in order to help maintain an optimal NFP. If the NFP drops too low (<10 mm Hg), kidney function stops.
Renal Physiology (cont) Blood pressure is the driving force for filtration but there are opposing forces at work. Filtration occurs through the filtration membrane. Fig. 10 a
Renal Physiology (cont) The glomerular filtration rate (GFR) is the amount of filtrate produced per minute (about 125 ml for 2 kidneys). About 10% of the fluid passing through the kidneys appears as filtrate (180 l / day) with 99% reabsorbed back into the blood. Regulating GFR is critically important. NFP = GHP – CsHP = 50 mmHg – 15 mmHg = 35 mm Hg FP = NHP – BCOP = 35 mmHg – 25 mm Hg = 10 mm Hg A decrease in glomerular blood pressure by only 20% will stop filtration. GFR is controlled by kidney autoregulation, neural mechanisms, and the RAA (renin-angiotensin- aldosterone) response to falling blood pressure.
Renal Physiology (cont) H2O and small solutes pass through the filtration membrane Fig. 10 b
Renal Physiology (cont) A number of tests are used to evaluate kidney filtration. The creatinine clearance test is used to estimate GFR. Creatinine is not reabsorbed from the filtrate so a comparison between blood and urine levels is calculated. If 84 mg of creatinine appears in the urine each hour and the plasma concentration is 1.4 mg / dl, the GFR = 84 mg/hr 1.4 mg/dl About 15% of the creatinine does enter by secretion so if more accuracy is required, inulin, a protein that is neither reabsorbed nor secreted, is administered to more accurately determine GFR. = 60dl / hr = 100 ml / min
Renal Physiology (cont) Autoregulation of GFR is achieved by adjusting the diameter of the afferent and efferent arterioles, glomerular capillaries and their supporting cells. If the systemic blood pressure declines, the following responses to maintain GFR occur. *the afferent arteriole dilates *supporting cells relax and capillaries dilate *the efferent arteriole constricts. If the systemic blood pressure rises, stretch of the afferent arteriole results in a reflex constriction of its smooth muscle cells which decreases blood flow to the glomerulus in order to regulate GFR.
Renal Physiology (cont) Hormonal regulation of GFR is due to the renin- angiotensin system and atrial natriuretic peptide. Renin is released from the JGA when renal blood flow declines or the osmotic concentration of the fluid in the DCT decreases (because flow slowed, more solutes were pumped out along the ascending loop of Henle). Angiotensin II *vasoconstricts peripheral systemic arterioles and precapillary sphincters *constricts the efferent arteriole and stimulates reabsorption of Na+ and H2O along the PCT *stimulates aldosterone release, thirst, ADH release, and peripheral sympathetic vasoconstriction
Renal Physiology (cont) Hormonal regulation of GFR (cont) In response to rising blood pressure, cells of the right atrium release ANP which causes *dilation of the afferent arteriole and constriction of the efferent arteriole to increase GFR and urine production Increased urine production lowers blood volume resulting in a decrease in blood pressure. Autonomic regulation of GFR is due to the sympathetic activation triggered by a sudden fall in blood pressure which vasoconstricts the afferent arteriole to decrease GFR temporarily (protecting vital organs). A similar response occurs during strenuous exercise.
Renal Physiology (cont) Regulation of GFR Fig. 11 b
Renal Physiology (cont) Reabsorption and Secretion along the renal tubule: Solutes that need to be retained in the body are reabsorbed from the filtrate and others that need to be removed from the body are secreted into the filtrate along the renal tubule. The transport mechanisms utilized by tubule cells include simple diffusion, facilitated diffusion, active transport, and two additional transport mechanisms that secondarily depend on the solute gradients set up by active transport—cotransport and countertransport. The rate of transport of a substance through a tubule cell depends on the number of carrier proteins present in its cell membrane on the apical and basolateral surfaces.
Renal Physiology (cont) The solute concentration at carrier saturation is the transport maximum (Tm). When the filtrate concentration of a substance exceeds the Tm, the remaining molecules of that substance will appear in the urine. The renal threshold is the plasma concentration of a substance when it begins to appear in the urine. The renal threshold for glucose is about 180 mg / dl and for amino acids it is about 65 mg / dl. Some substance are not transported by tubule cells so they always appear in the urine. TABLE 3 lists various substances in relation to renal transport.
Renal Physiology (cont) Osmolarity refers to the number of solute particles in a fluid. Osmolarity is expressed in osmoles per liter (Osm/l) or milliosmoles per liter (mOsm/l). A one Osm/l solution has one mole (grams = to molecular weight) of a dissolved solute in a liter of solvent. Most body fluids, including blood, have an osmotic concentration of about 300 mOsm/l. Each 1 mOsm/l = 19.3 mm Hg osmotic pressure Ion concentrations reported in millequivalents per liter are based on the number of cations and anions in solution. For substances with a single charge, a one mOsm/l solution is also a 1 mEq/l solution.
Renal Physiology (cont) osmotic concentrations of the blood and filtrate Fig. 16 47
Renal Physiology (cont) Cells of the initial portion of the renal tubule, the PCT, are responsible for reabsorbing *around 70% of the filtrate volume, *all of the glucose, amino acids, and other nutrients, *many solutes including Na+, K+, Ca2+, bicarbonate ions, and others. PTH stimulates Ca2+ reabsorption. PCT cells also actively secrete H+. Active transport of Na+ at the basolateral surface sets up the gradient for reabsorption of Na+ coupled to the secretion of H+ using a countertransport protein and with the reabsorption of glucose using a cotransport protein on the apical surface of PCT cells.
Renal Physiology (cont) Transport along the PCT microvilli present note how Na+ is reabsorbed by several types of transport proteins absorption of CO2 from tubular fluid provides for reabsorption of bicarbonate ions and secretion of H+ pump Fig. 12
Renal Physiology (cont) Loop of Henle and Countercurrent Exchange Of the remaining filtrate entering the loop of Henle, ½ of the water and ⅔ of the Na+ and Cl– ions will be reabsorbed through its specialized cells. Water is reabsorbed from the filtrate as it passes down the descending limb of the loop of Henle and Na+ and Cl– are reabsorbed by active transport across the cells of the ascending limb of the loop of Henle to produce a filtrate with a solute concentration ⅓ that of the plasma. The descending limb is permeable to water and impermeable to solutes. The thick ascending limb is impermeable to water and solutes but has ion transporters powered by many Na+/ K+ exchange pumps on the basolateral surface.