Study Design
Randomized phase III trial of trabectedin versus doxorubicin-based chemotherapy as first-line therapy in translocation-related sarcomas (TRS).

Study Design
E N D
Presentation Transcript
Randomized phase III trial of trabectedin versus doxorubicin-based chemotherapy as first-line therapy in translocation-related sarcomas (TRS) Sant P. Chawla, Andrew Hendifar, Michael Leahy, Antoine Italiano, Shreyaskumar Patel, Peter Hohenberger, Armando Santoro, Arthur P. Staddon, Nicolas Penel, Sophie Piperno-Neumann, Pilar Lardelli, Antonio Nieto, Carmen Kahatt, Jean-Yves Blay
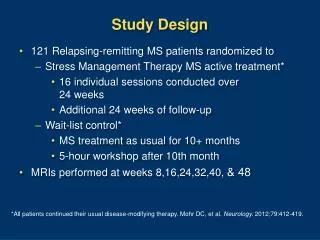
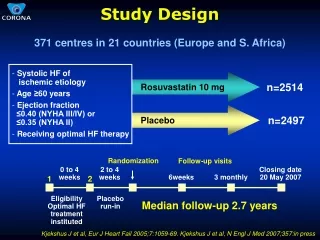
Eligible patients MRCL (n= 40) Other TRS (n= 40) PS= 0 PS= 1-2 PS= 0 PS= 1-2 RANDOMIZATION (1:1) Study Design • An adaptive design in chemonaïvepatients with advanced TRS, stratified by performance status and subtype, then randomized to receive: • Trabectedin: 1.5 mg/m2 in 24h iv infusion q3wk • Doxorubicin based chemotherapy (DXCT): single agent 75 mg/m2 q3wk, or 60 mg/m2 combined with ifosfamide 6-9 g/m2 q3wk
Study Objectives • Primary: Progression free survival (PFS) of trabectedinvs DXCT • Secondary: • PFS at 6 months • Response rate (RR) • Overall survival • Safety • PFS/RR analyzed by investigator assessment for all randomized patients • PFS/RR analyzed by independent review only for confirmed TRS patients
Results: Baseline Characteristics Trabectedin (n=61) DXCT (n=60) Age (yr) Median (range) 47 (19-78) 49 (19-78) Sex Male / female 36 (59%) / 25 (41%) 38 (63%) / 22 (37%) ECOG PS 0 28 (46%) 29 (48%) 1 32 (52%) 30 (50%) 2 1 (2%) 1 (2%) Sarcoma type by Investigator MRCL 28 (46%) 28 (47%) Other 33 (54%) 32 (53%) Sarcoma type by central pathology MRCL 23 (38%) 17 (28%) Other 28 (46%) 20 (33%) Not confirmed* 10 (16%) 23 (38%) * Wrong diagnosis 4 (7%) and 9 (15%) patients of the trabectedin and DXCT arms, no evidence of translocation in 3 (5%) and 2 (3%) patients, and lack of available material for central review in 3 (5%) and 12 (20%) patients
Histology According Central Diagnosis (TRS Confirmed Patients N=88)
Results: Baseline Characteristics Trabectedin (n=61) DXCT (n=60) Disease Extension Locally advanced 18 (30%) 13 (22%) Metastatic 43 (70%) 47 (78%) 33 (54%) 38 (63%) Prior surgery (radical/palliative) 24 (39%) Prior radiotherapy 21 (35%) Number of sites involved at baseline, Median (range) 2 (1-5) 2 (1-8) Months from first diagnosis to randomization, Median (range) 10 (1-187) 8 (0-310)
Censoring • A high percentage of patients were censored in both arms • Main reasons for censoring: • Surgical removal of lesions • 24% in trabectedin arm and 16% in the DXCT arm • Administration of a new anticancer therapy (chemotherapy or radiotherapy) before progression of the disease • 18% in trabectedin arm and 24% in DXCT arm • Importantly, 35-40% patients in either arm ended up receiving the drug in the other arm • Patients in trabectedin arm also received DXCT • Patients in DXCT arm also received trabectedin
Median: 16.1 months (95% CI, 5.5-21.9) Median: 8.8 months (95% CI, 5.5-12.7) Hazard ratio: 0.85, p=0.5551. Log rank p=0.5533 Results: PFS by Investigators
Median:18.8 months (95% CI, 5.7-not reached) Median: 8.3 months (95% CI, 7.1-25.0) Hazard ratio: 0.86; p=0.6992. Stratified log-rank p=0.9573 Results: PFS by Independent Review
Median: 38.9 months (95% CI, 24.2-nr) Median: 27.3 months (95% CI, 21.3-39.6) Hazard ratio: 0.77, p=0.3672. Log rank p=0.3659 Results: Overall Survival
OS in MyxoidLiposarcoma Median: 95% CI (-) Median: 33.1 95% CI (21.2-39.6) Hazard ratio: 0.25, p=0.0453. Log rank p=0.0314
Summary • The study was underpowered to detect any statistical significant differences in the two arms due to high rate of censoring in both arms • Overall, no statistically significant differences in PFS/OS were observed • Median PFS was 19 mo. in trabectedin arm vs. 8 mo. in DXCT arm • Median OS was 39 mo. in trabectedin arm vs. 27 mo. in DXCT arm • Safety profiles for trabectedin and DXCT were consistent with previous studies • Ability to administer trabectedin over prolonged periods without cumulative toxicity may allow for longer disease control • Trabectedin should be further explored in a definitive randomized study in myxoidliposarcoma patients
Discontinuations and Dose Reductions • Administrationdelays and dosereductionsoccurred more frequently in thetrabectedinarm, partiallyduetotheprolongedtreatmentduration. • Transaminaseincreasewasthemainreasonfordosereduction • Neutropenia wasthemostcommon cause of administrationdelay.