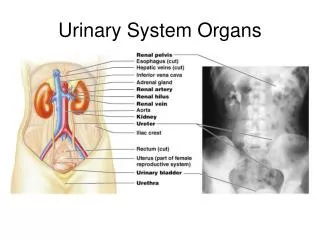
Urinary System Organs
Urinary System Organs. Kidney Functions. Filter 200 liters of blood daily allowing removal of toxins an metabolic wastes (urea, lactic acid, ammonia, H + ) from the blood

Urinary System Organs
E N D
Presentation Transcript
Kidney Functions • Filter 200 liters of blood daily allowing removal of toxins an metabolic wastes (urea, lactic acid, ammonia, H+) from the blood • Regulate volume and chemical makeup of the blood by altering water and electrolyte excretion. i.e. K+, Na+, Cl-, Ca2+ • Maintain the proper balance acid/base balance by regulating levels of : H+ and HCO3- • Production of renin to help regulate blood pressure • Erythropoietin to stimulate RBC production • Activation of vitamin D which will be important for calcium absorption in bone.
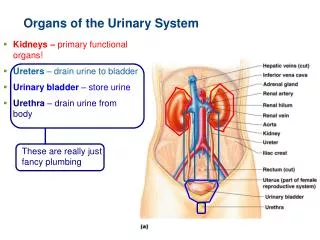
Urinary System Anatomy • 2 Kidneys are located in the abdominal cavity ( retroperitoneal) on either side of the spinal cord. • It is found on the posterior abdominal wall between T12- L3 The renal hilum is the location were the major vessels enter or exit the kidney. • renal arteries supplies blood to the kidneys • blood leaves the kidneys by the renal veins • urine leaves the kidneys by the ureters • temporarily stored in the bladder
Kidney Anatomy - Internal • 3 distinct regions • Renalcortex • outermost layer • Renal medulla • middle layer consisting of cone-shaped medullary pyramids • Renal pelvis inner most layer • collect urine and funnel it to the ureter
The Nephron • Nephrons are the structural and functional units that form urine, consisting of: • Renal corpuscle : Glomerulus and Bowman’s capsule. • location where filtrate is formed. • Renal tubule: a long convoluted tube that re-absorbs substances that the body needs and excretes materials it wants to eliminate. • Each kidney contains approximately 1.2 million nephrons
Urine Formation • The kidneys filter the body’s entire plasma volume 60 times each day. • Over 99% of the plasma that is filtered will be reabsorbed from the renal tubules back into the peritubular capillaries and vasa recta. • Approximately 1.5 liters daily will not be reabsorbed. • The result is urine which will to be collected in the bladder.
Ions, water and smaller solutes .i.e. sugar can pass through the glomerular membrane. • Larger molecules such as blood cells and plasma proteins will not normally be part of filtrate unless some underlying pathology was present. • Hypertension
Renal Tubule • Divided into 4 major regions • Proximal convoluted tubule (PCT) – composed of cuboidal cells with numerous microvilli • Reabsorbs water and solutes from filtrate collected in bowman's capsule. 65-75 % of filtrate is re-absorbed here. • The body also secretes substances for elimination here. • Loop of Henle • Descending Loop of Henle extends from the cortex to the medulla • Permeable to water • Ascending Loop of Henle returns from the medulla to the cortex • Permeable to solutes • Distal tubule • located in cortex • Permeable to both water and solutes • Influenced by several hormones. • Collecting duct • descends from the cortex through the medulla where the concentrated filtrate can enter the renal pelvis • From here it will be funneled to the ureters • Permeable to both water and solutes.
Capillary Beds of the Nephron • Every nephron has two capillary beds • Glomerulus • Renal artery enters the kidney which branches and becomes smaller until its considered an afferent arteriole that will enter into the Bowman’s capsule. The vessel that is packed in this capsule is the glomerulus: • Peritubular Capillaries. • Each glomerulus is drained by a smaller efferent arteriole which becomes peritubular capillaries. • These will then wrap around the collecting ducts • Wrap around the loop of Henle via the vasa recta :
Reabsorption in the PCT • Sodium reabsorption is primarily by active transport • Na+ enters the renal tubular cells by secondary active transport. • This will be the driving force to reabsorb other nutrients such as glucose, amino acids and some vitamins and electrolytes ( Na, K, Cl, HCO3-, Ca2+…) • Many are taken into the cells with Na+ (symport) same direction. • In order to keep the Na+ concentration low in the renal cells Na+-K+ ATPase pumps Na+ out of the basilar membrane of the cell. • Water follows solvents such as Na+ by osmosis • Fat-soluble substances can easily diffuse from the renal tubule to the blood.
Mechanisms of Reabsorption in the Proximal Convoluted Tubule
Loop of Henle: • The descending loop of Henle: (DLH) High concentration of aquaporins making it very permeable to water and impermeable to solutes such as Na+ • As the water follows its osmotic gradient out of the DLH to the renal medulla the concentration of solutes inside the tubule increases from 300 mOsm ( = To blood plasma) to 1200 mOsm deep into the medulla. • The ascending loop of Henle: (ALH) is permeable to solutes and impermeable to water. • Since the tubule osmolarity is high (1200 mOsm) NACL will at first diffuse out of the tube to the renal medulla. As you go further up to the thick part of the ALH active transport will be needed to actively pump out NACL. • This reduces the osmolarity in the renal tubule from 1200 to 100 mOsm )
Osmotic Gradient in the Renal Medulla Figure 25.13
Tubular Secretion • Essentially reabsorption in reverse, where substances move from peritubular capillaries or tubule cells into filtrate • Tubular secretion is important for: • Disposing of substances not already in the filtrate • Eliminating undesirable substances such as urea and uric acid • Ridding the body of excess potassium ions • Controlling blood pH monitoring levels of both H+ HCO3-
Renal Regulation of body pH • The kidneys work in conjunction with the respiratory system to regulate the pH of the body. • Respiratory: both rate and membrane health can influence H+ concentration in the blood. • A reduction in breathing rate or impaired respiratory membrane increase H+ (acidosis) • Reduction of CO2 in the body following hyperventilating results in a increase pH (alkalosis) • Metabolic changes in pH can result from cellular metabolism or ingestion of a substance. • It controls the the amount of H+ and HCO3- that are excreted or reabsorbed based on the current pH of the body.
Renal Regulation of pH • If the pH is low (acidosis)the kidneys will: • Eliminate excess H+ and reabsorbing and producing additional HCO3- to increasing pH as needed. • If the pH is high (alkalosis) the kidneys respond by: • reabsorbing H+ and not reabsorbing or producing additional HCO3- . • How will a patient with chronic emphysema present: • Respiratory and renal response • How will a patient in diabetic ketoacidosis present: • Respiratory and renal response • How will a patient who swallowed a bottle of baking soda present: • Respiratory and renal response
Urinary Bladder • Ureters enter the base of the bladder through the posterior wall • The bladder wall has three layers • Transitional epithelial mucosa • A thick muscular layer • A fibrous adventitia • The bladder is distensible and collapses when empty • Can hold 700-800 cc of urine before the urge to urinate • Urine is 95% water and 5% solutes • Nitrogenous wastes i.e. urea • Other normal solutes include: • Sodium, potassium, phosphate, sulfate, calcium, magnesium, bicarbonate and hydrogen ions • Abnormally high concentrations of any urinary constituents may indicate pathology
Micturition (Voiding or Urination) • Urinary Retention :Sympathetic Nervous System • Distension of bladder walls initiates spinal reflexes that: • Stimulate contraction of the external urethral sphincter and internal sphincter • Inhibit the detrusor muscle (temporarily) • Voiding reflexes: Parasympathetic Nervous System • Stimulate the detrusor muscle to contract • Inhibit the internal( involuntary) and external(voluntary)sphincters • Sympathetic stores/ Parasympathetic pours
Glomerular Filtration • The glomerulus is more efficient than other capillary beds because: • Its filtration membrane is significantly more permeable • Glomerular blood pressure is higher • Afferent arterioles have larger diameters than efferent arterioles resulting in a back pressure. • This results in a higher net filtration pressure • Fluids and solutes are forced out of the blood throughout the entire length of the glomerulus • Plasma proteins are not filtered and are used to maintain oncotic pressure of the blood
Glomerular Filtration Rate • The total amount of filtrate formed per minute by the kidneys • GFR = 125 ml/min or 180 L/day, male • GFR = 105 ml/min or 150 L/day, female • Filtration rate is directly proportional to • Total surface area available for filtration • Filtration membrane permeability • Net filtration pressure • Changes in GFR normally result from changes in glomerular blood pressure
Renal Autoregulation of GFR • Myogenic mechanism • Self regulating mechanism if BP is less than 160 mmHg • BP stretches afferent arteriole afferent arteriole constricts dilate efferent • restores GFR • BP dilate afferent arteriole, constrict efferent • restores GFR
Juxtaglomerular Apparatus (JGA) • Specialized cells located where the distal tubule lies against the afferent arteriole. • If there is a decrease in systemic blood pressure: • less blood will be filtered in the glomerulus. • Decrease in GFR results. • The JG cells of the kidneys will respond by producing renin.
Renin Release • Renin release is triggered by: • Reduced blood flow in the afferent arterial there is reduced stretch of the JG cells • Macula densa cells of the DCT monitor Na+ ion concentration. • When there is less filtrate formed in the Bowman’s capsule a higher % of the solutes such as Na+ will be reabsorbed in PCT and ALH. • This creates a hypotonic filtrate in the DCT. • triggering chemoreceptors that will cause the release of renin.
Renin-Angiotensin Mechanism • Renin acts on an inactive plasma protein angiotensinogen resulting in angiotension I • Angiotensin I circulates in the blood until it gets to the lungs. • ACE enzyme (Angiotension Converting Enzyme) in the lungs converts Angiotension I to angiotensin II • Angiotensin II increases blood pressure by 3 mechanisms: • Stimulates the hypothalamus making you thirsty. • Acts as a potent vasoconstrictor which causes arterial pressure to rise. • Stimulates the adrenal cortex to release aldosterone that increases Na+ ion reabsorption • Both systemic and glomerular hydrostatic pressure rise • Ace inhibitors block the conversion of Angiotensin I to angiotensin II thus will lower blood pressure.
ACE Inhibitors • Renin- Angiotensin system can have detrimental effects on the failing heart or someone with chronic hypertension. • Excessive vasoconstriction increases peripheral vascular resistance increases (after load) which can decrease LV function and cardiac output. • Salt and water retention from Aldosterone can increase ventricular volume (pressure).(Preload). • ACE inhibitors block the conversion of angiotension I to angiotension II thus eliminating these potential side effects .
Blood and Nerve Supply • Kidneys are .5% of the body weight • Receive 21% • (1200 ml) of systemic cardiac output each minute. • The nerve supply is via the superior mesenteric plexus • Consists of mostly sympathetic fibers
SNS and Renal Blood flow. • Under stress norepinephrine is released by the SNS and epinephrine by the adrenal medulla. • Both cause afferent arterioles constrict and filtration is reduced in an effort to shunt the blood to the heart lungs, brain and muscles necessary to deal with the stress. • The sympathetic nervous system also stimulates the renin-angiotensin mechanism. • Direct stimulation of the JG cells via 1-adrenergic receptors by renal nerves. • Renal Failure can occur due to excessive stimulation of SNS or hemorrhage. • This results in a severe drop in blood flow to renal tissue. • Hypoxia and tissue death can result.
Distal Tubule (DT) and Collecting Duct (CD) • Regulate blood pressure pH, water and electrolyte concentration in the body. • Dependent upon certain hormones. • Antidiuretic Hormone (ADH) and Aldosterone are released when systemic blood pressure is low. • Atrial Natriuretic Hormone (ANH) is released from the heart when blood pressure is high.
Hormonal Control of Blood Pressure • ADH is triggered by prolonged fever; excessive sweating, vomiting, or diarrhea; severe blood loss; and traumatic burns. • Hypothalamic osmoreceptors trigger or inhibit ADH release. • When osmolarity is high (dehydration) it will be released. • Osmolarity is low( Excessive fluids) it will be inhibited. • ADH stimulates aquaporins to reabsorb water in the DCT and CD. • Low ADH levels produce dilute urine. • Diabetes insipidus • High ADH levels produce concentrated urine • In high concentration also acts as a arterial vasoconstrictor
Hormonal Control of Blood Pressure • Aldosterone acts on the ALH and DT/ CD • increases Na+ reabsorption and K+ secretion • BP increases as water follows its osmotic gradient. • Aldosterone secretion is stimulated by: • Rising blood levels of K+ • Low blood Na+ • Decreasing blood volume or pressure • Atrial Natriuretic Peptide (ANP): released by the atria of the heart in response to increased venous return as seen with high BP. • Increases both the secretion of salt and water in the urine by: • decreases Na+ permeability of the CD which will increase urine production thus lowering BP • It will also inhibit Aldosterone release • Inhibits the renin-angiotensin- mechanism • Dilates the afferent arterial and constricts the efferent thus increasing GFR
Diuretics • Chemicals that enhance the urinary output reducing cardiac preload. • Osmotic diuretics include: • High glucose levels – water follows the tubular glucose out in the urine. • Alcohol – inhibits the release of ADH • Caffeine and most diuretic drugs – inhibit sodium ion reabsorption • Lasix and Diuril – inhibit Na+-associated symporters (Block Na reabsorbing)