Monte Carlo Simulation
Monte Carlo Simulation. G.L. Drusano, M.D. Co-Director Ordway Research Institute & Research Physician New York State Department of Health Professor of Medicine & Pharmacology Albany Medical College. Monte Carlo Simulation. Monte Carlo simulation was invented by Metropolis and von Neumann

Monte Carlo Simulation
E N D
Presentation Transcript
Monte Carlo Simulation G.L. Drusano, M.D. Co-Director Ordway Research Institute & Research Physician New York State Department of Health Professor of Medicine & Pharmacology Albany Medical College
Monte Carlo Simulation • Monte Carlo simulation was invented by Metropolis and von Neumann • This technique and its first cousin Markov Chain Monte Carlo have been used since for construction of distributions (Markov Chain Monte Carlo was actually described as a solution to the “simulated annealing problem” in the Manhattan Project –Metropolis et al)
Monte Carlo Simulation • The first use of Monte Carlo simulation for drug dose choice and breakpoint determination was presented on October 15, 1998 at an FDA Anti-Infective Drug Products Advisory Committee • At this time, the drug was presented as “DrugX” but was evernimicin • The ultimate outcome was predicted by the method (but the drug died)
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Required Factors for Rational Dose/Drug Comparison 1. Pharmacodynamic Goals of Therapy 2. Population Pharmacokinetic Modeling 3. Target Organism(s) MIC Distribution 4. Protein Binding Data in Animal and Man
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
Role of Monte Carlo Simulation for Dose Choice for Clinical Trials of Anti-Infectives Drusano GL, SL Preston, C Hardalo, et al. Antimicrob Agents Chemother. 2001;45:13-22.
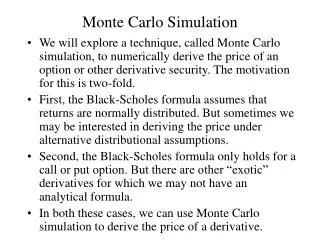
Monte Carlo Simulation • What is Monte Carlo simulation, as applied to Infectious Diseases issues? • What are the technical issues? • For what is Monte Carlo simulation useful?
Monte Carlo Simulation • What is Monte Carlo simulation? MC simulation allows us to make use of prior knowledge of how a target population handles a specific drug to predict how well that drug will perform clinically at the dose chosen for clinical trials and to rationally set breakpoint values for susceptibility
Monte Carlo Simulation • How is this done? Through use of the mean parameter vector and covariance matrix, derived from a population PK study, a sampling distribution is set up. This allows the peak concentrations, AUC and Time > threshold to be calculated for all the subjects
Monte Carlo Simulation • How do we use this to predict the clinical utility of a specific drug dose? 1) Identify the goal of therapy (cell kill, resistance suppression, etc) 2) Identify the sources of variability that affect achieving the goal of therapy a) PK variability (accounted for by MCS) b) Variability in MIC’s (or EC95, etc) c) Protein binding (only free drug is active)
Monte Carlo Simulation • What do we do? As an example, for a drug that is AUC/MIC driven in terms of goal of therapy (e.g. AUC/MIC of 100 for a good microbiological outcome), we can now take the 2000 (or 10000 or whatever) simulated subjects and divide the AUC by the lowest MIC in the distribution, then determine how many achieve the target of 100. This is then repeated with higher MIC values until the target attainment is zero or some low number
How does this help evaluate the utility of a specific drug dose? We have target attainment rates at each MIC value in the organism population distribution. A specific fraction of the organisms have a specific MIC. A weighted average for the target attainment rate (taking an expectation) can be calculated. This value will be the overall “expected” target attainment rate for the outcome of interest for that specific dose. Monte Carlo Simulation
Monte Carlo Simulation Technical Issues
Monte Carlo Simulation • What are the factors that may affect the simulation? ►Model mis-specification ►Choice of distribution ►Covariance matrix (full vs diagonal) ►Simulating the world from 6 subjects
Monte Carlo Simulation Model Mis-specification
Monte Carlo Simulation • Model mis-specification Sometimes, data are only available from older studies where full parameter sets and their distributions were not reported • Some investigators have used truncated models for simulation (1 cmpt vs 2 cmpt) • This may have more effect for some drugs relative to others (β lactams vs quinolones)
Monte Carlo Simulation Choice of Distribution
Monte Carlo Simulation • There are many underlying distributions possible for parameter values • Frequently, there are insufficient numbers of patients to make a true judgement • One way to at least make the choice rational is to examine how one distribution vs another recapitulates the mean parameter values and measure of dispersion • A quinolone example follows (N vs Log-N)
Monte Carlo Simulation • Here, it is clear that the Log-normal distribution better recaptures the mean parameter values and, in general, the starting dispersion (except Kpc) • And for AUC distribution generation, it is clear that Log-normal is preferred because it performs better for the parameter of interest (SCL) for both mean value and dispersion • We have seen examples where there is no substantive difference (N vs Log-N)
Monte Carlo Simulation Full vs Major Diagonal Covariance Matrix
Monte Carlo Simulation • Sometimes, only the population standard deviations are available and only a major diagonal covariance matrix can be formed • Loss of the off-diagonal terms will generally cause the distribution to become broader (see example) • One can obtain an idea of the degree of impact if the correlation among parameters is known (of course if this is known, one could calculate the full covariance matrix!)
Monte Carlo Simulation Mean = 139.6 Median = 120.2 SD = 82.4 95% CI = 41.2-348.8 Mean = 140.4 Median = 121.4 SD = 83.5 95% CI = 40.7-351.4
Monte Carlo Simulation Simulating the World From 6 Subjects
Monte Carlo Simulation n = 6 n = 25 n = 50
Monte Carlo Simulation • Obviously, the robustness of the conclusions are affected by the information from which the population PK analysis was performed • If the “n” is small, there may be considerable risk attendant to simulating the world • One of the underlying assumptions is that the PK is reflective of that in the population of interest – care needs to be taken and appropriate consideration given to the applicability of the available data to the target population
Monte Carlo Simulation • But, in the end, something is probably better than nothing, so simulate away, but interpret the outcomes conservatively • It is also important to examine the SD’s, as drawing inferences on drug dose from volunteer studies, where CV%’s are sometimes circa 10% may be risky • How many simulations should be done? - Answer: as always, it depends • To stabilize variance in the far tails of the distribution (> 3 SD), it is likely that one would require > 10000 simulations
Monte Carlo Simulation • Utility of Monte Carlo simulation, a non-exhaustive list: ► Determination of drug dose to attain a specific endpoint ► Determination of a breakpoint ► Examine variability in drug penetration
Monte Carlo Simulation Some New Stuff: • Effect simulations for combinations • Use of estimated GFR in simulations • Identification of a resistance-counterselective dose
Monte Carlo Simulation Hope W et al. J Infect Dis 2005;192:673-680.
Monte Carlo Simulation Greco Model for Combination Chemotherapy Hope W et al. J Infect Dis 2005;192:673-680.
Monte Carlo Simulation Greco Model for Combination Chemotherapy Hope W et al. J Infect Dis 2005;192:673-680.
Monte Carlo Simulation Hope W et al. J Infect Dis 2005;192:673-680.
Monte Carlo Simulation 5-FC 30 mg/Kg/day Amphotericin B 1 mg/Kg/day 5-FC 30 mg/Kg/day Amphotericin B 0.6 mg/Kg/day 5-FC 30 mg/Kg/day Amphotericin B 0.3 mg/kg/day
Monte Carlo Simulation • It is straightforward to model combinations of agents • Our laboratory has also done so for anti-retrovirals • For Amphotericin B/5-FC, it is clear that the current dose of 5-FC is far too large (at least for C. albicans) and only adds toxicity • Monte Carlo simulation shows that use of 30 mg/Kg 5-FC with Ampho B doses as low as 0.3 mg/Kg gives up little effect, but would have significantly diminished toxicity
Population Pharmacokinetic Parameter Values for Ceftobiprole
Observed vs. Predicted Plot after the Bayesian Step Observed = 1.003 x Predicted + 0.627; r2 = 0.947; p << 0.001
Target Attainment Probabilities for a 500 mg dose of ceftobiprole administered as a 1 hour, constant rate intravenous infusion every 12 hours. Target was maintaining free drug concentrations in excess of the MIC for 30% of the dosing interval. Estimated creatinine clearances were held constant for each analysis at the indicated values between 20 ml/min and 120 ml/min.