Download
1 / 36
370 likes | 594 Vues
Out of sight out of mind: Brain Impairment and HIV. Victor Valcour MD Associate Professor Memory and Aging Center University of California – San Francisco/ USA. Brain Impairment and HIV. Cognitive impairment remain frequent despite HAART Causes of brain:

E N D
Out of sight out of mind: Brain Impairment and HIV Victor Valcour MD Associate Professor Memory and Aging Center University of California – San Francisco/ USA
Brain Impairment and HIV • Cognitive impairment remain frequent despite HAART • Causes of brain: • Current treatment approaches do not clear reservoirs • Co-existing factors (treatment complications/side effects, other diseases, non-HIV related issues) • Aging with HIV • Should we be worried about neurological degenerative disorders (Alzheimer’s? Parkinson's?)
21% Developed impairment after 48 weeks of HAART Brain Impairment and HIV 22% Mildly Impaired 39% Impaired 17% Moderately Impaired Robertson K, et al. AIDS. 2007
Cognitive Impairment despite HAART Pre- ARV Pre-HAART HAART Grant et al. 2009 Conference on Retroviruses and Opportunistic Infections
Neuropsychological Impairment in the era of HAART (2007) HIV Asymptomatic Neurocognitive Impairment Mild Neurocognitive Disorder HIV infection without cognitive impairment HIV-associated Dementia Consensus Working Group, Neurology 2007
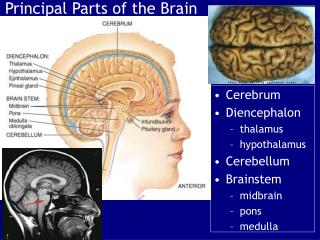
Clinical Features Cognition Memory loss Concentration Mental slowing Comprehension Behavior Apathy Depression Agitation, mania Motor Unsteady gait Poor coordination Tremor
Functional consequences of cognitive impairment in HIV Heaton et al JINS 2004
The Case of Mr. B • 79 year old male, high school degree, held miscellaneous jobs • Referred for research project studying aging • “would be a good control subject…has no cognitive problems” • Participant -asymptomatic • “I like opera and I used to be able to name all the singers…a lot of it escapes me now”
Mr. B’s HIV history • HIV+ since 1985 • Asymptomatic for decades but eventually started HAART in 2001 with CD4~200 • No opportunistic infections; mild neuropathy • Currently plasma HIV RNA level – undetectable • Current CD4 ~ 250 • Has not had detectable viral load or CD4 less than 200 since 2001
Mr. B’s other medical issues • Past Medical History • hepatitis A (1960); occasional vertigo, intermittent illicit drug use including methamphetamine (last use at 75 years old) • Neurological exam abnormal • Increased reflexes, slowed finger tapping, distal symmetric neuropathy, abnormal eye movements • Neuropsychological deficits broadly and severe
Why is this occurring? Is HAART sufficient? What is the role of coexisting morbidity?
HIV (1) HIV-infected monocytes, some activated HAART (5) Altered integrity of the BBB facilitating further transmigration of infected M/MФ (2) Transfer of HIV into the brain - infection establishment in perivascular macrophages (3) Impacts brain cells leading to cognitive dysfunction (4) Neuronal dysfunction and death Pathology demonstrates multinucleated infected cells (perivascular monocytes), little neuronal infection, but dysfunctional neurons with decreased arborization and damaged synaptic function Capillary lumen Blood Brain Barrier
Peripheral monocyte infection correlates to HIV dementia Poorer cognitive performance Valcour Neurology 2009
Failure of HAART to eradicate virus in circulating monocytes Valcour et al, J Leukocyte Biology 2010
Correlation between HIV DNA and cognition in treated subjects All Individuals Individuals with undetectable plasma HIV RNA Not Impaired Impaired Not Impaired Impaired Shiramizu, et al 2005 AIDS
CD68 expression in hippocampusElevated despite viral control with HAART Anthony, Bell, et al. J Neuropath Exp Neurol 2005
(1) HIV-infected monocytes, some activated HAART ? (5) Altered integrity of the BBB facilitating further transmigration of infected M/MФ (2) Transfer of HIV into the brain - infection establishment in perivascular macrophages (3) Impacts brain cells leading to cognitive dysfunction (4) Neuronal dysfunction and death Capillary lumen Blood Brain Barrier
CPE and CSF viral load Proportion with detectable virus in CSF HAART with higher BBB penetration Letendre et al 2008 Arch Neurol
Non-HIV specific Contributors to Cognitive Impairment in HIV
Smoking Younger Older 21% 42% Cerebrovascular risks Hypertension Younger Older 43% 47% 12% 26% 2% 7% Diabetes Younger Older FG 100-125 15% 25% FG > 125 or DM 3% 22% JNC7 Deaths in the Hawaii Aging with HIV Cohort Undetermined Cardiovascular 21.05% 21.05% Drug overdose 10.53% Cancer 21.05% Liver failure 5.26% HAART related lactic AIDS-related acidosis 10.53% 10.53%
Cognitive performance worse with greater number of cerebrovascular risk factors
The role of Co-existing Morbidity • Cerebrovascular disease • Carotid Intimal Medial Thickness correlates to cognitive performance in the Multicenter AIDS Cohort Study (MACS) • Other non-HIV specific factors • Illicit drug use • Co-infections, particularly Hepatitis C • Depression and other psychiatric conditions Becker 2010 Neurology and Valcour 2005 JAIDS
Aging with HIV infection The Honolulu Advertiser 2003 The New York Times January 2007
Prevalence of Dementia % of population
Prevalence of Dementia % of population
Amyloid accumulation Amyloid degradation Amyloid deposition in HIV
Amyloid accumulation Amyloid degradation Amyloid deposition in HIV • Inflammation (Alisky 2007) • Metabolic syndrome (Giunta 2008) • IFNg, TNFa (Liao 2004, Cu 2008) • Ubiquitin proteosome dysfunction due to HAART (Clifford 2007) • Gamma secretase impairment due to immune activation (Brew 2005) • Increased APP as an acute phase reactant (Xu 2008) • GP41 inhibitions of protein kinase C ((Ikezu 2008) • Tat inhibition of micoglial uptake of amyloid beta (Giunta 2008) • Tat interactions with low density lipoprotein receptor inhibiting uptake of amyloid (Liu 2000) • Protease inhibitor down-regulation of insulin degradation enzyme which degrades amyloid • Tat interactions with neprolysin, inhibiting amyloid degradation (Rempel & Pulliam, 2005) • TNFa stimulated BACE1 suppressing amyloid beta degradation in microglia (Xu 2008) • Sub-lethal HIV mediated NMDA excitations leading to alpha secretase inhibition (Xu 2008)
Good news • No evidence for increased fibrillary amyloid plaque in well-controlled HIV Ances, Clifford 2010 • Damage to neuron synapses and decreased arborization of neurons appears to be reversible Ellis, Masliah, 2008
UCSF HIV Over 60 Cohort Abstract # 11302, IAS 2010
Where do we go from here? • HIV cognitive impairment remains a silent epidemic • Although dementia is rare, milder levels of impairment are frequent and impact function • Many patients adopt compensatory means of getting by • Work is needed to detect and treat these issues
Where do we go from here? • HIV appears to be inadequately treated within current treatment approaches • Sequestered reservoirs are inadequately treated – monocytes • Not all antiretroviral medications adequately get into the brain • More information is needed, but early data suggest this is a problem for some patients • Work is needed to address treatment of reservoirs
Where do we go from here? • Confounding factors are likely to emerge as important treatable aspects of cognitive impairment • Illicit drug use, cerebrovascular risk factors, hepatitis C, medication effects, sleep apnea, others • Patients and doctors should address these issues aggressively • Patients should remain physically and socially engaged
Where do we go from here? • There are theoretical concerns for the emergence of increased risk for neurodegenerative disorders in older HIV patients • It is too early to make firm conclusions at this time • More research is needed
Research support R01 NS061696 (Monocyte HIV DNA and HIV Dementia) K23AG032872 (Brain Impact of Aging with HIV) R21-MH086341 (Neurological Complications of Acute HIV Infection) UCSF AIDS Research Institute (NeuroImaging Correlates to Dementia in HIV over 60) UCSF-GladstoneCenter for AIDS Research (NeuroImaging Correlates to Dementia in HIV over 60) Hillblom Foundation (Cognitive Impact of Insulin Resistance in Aging HIV Patients) Thank you Special Thanks: Bruce Miller and the Memory and Aging Center Cecilia Shikuma, Bruce Shiramizu and the Hawaii Center for AIDS Jintanat Ananworanich and the Southeast Asia Research Collaboration with Hawaii (SEARCH, www.SEARCHThailand.org) Our research subjects in California, Hawaii and Thailand Disclosures: Dr. Valcour has provided consultative services to GlaxoSmithKline, Merck, and Abbott