Download
1 / 16
160 likes | 291 Vues
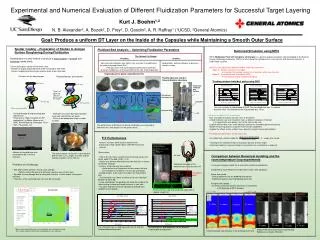
Psychosocial and behavioral correlates of STD and HIV risk behavior among Massachusetts men who have sex with men with symptoms of posttraumatic stress disorder. Sari L. Reisner, MA 1 , Matthew J. Mimiaga, ScD, MPH 1,2 ,

E N D
Psychosocial and behavioral correlates of STD and HIV risk behavior among Massachusetts men who have sex with men with symptoms of posttraumatic stress disorder Sari L. Reisner, MA1, Matthew J. Mimiaga, ScD, MPH1,2, Ashley M. Tetu, BS1,3, Kevin Cranston, MDiv4, David S. Novak, MSW4, Kenneth H. Mayer, MD1,5 1The Fenway Institute, Fenway Community Health, Boston, MA 2Harvard Medical School/Massachusetts General Hospital, Boston, MA 3Boston University, School of Public Health, Boston, MA 4The Massachusetts Department of Public Health, Boston, MA 5Brown Medical School/Miriam Hospital, Providence, RI
Background: Epidemiology of STDs and HIV in Massachusetts • Similar to national trends, Massachusetts men who have sex with men (MSM) continue to be at increased risk for STDs, including HIV. • Massachusetts trends: • MSM accounted for the majority of infectious syphilis cases, ranging from 68% in 2001 to 72% in 2005. • A 32-fold increase in Quinolone-resistant Neisseria gonorrhoeae (QRNG) was observed among MSM (two cases in 2001 and 66 cases in 2005). • Among males, the proportion of HIV cases with MSM exposure increased from 41% in 1999 to 54% in 2005.
Background: Psychosocial problems and sexual risk • Several studies have documented the association of psychosocial problems with sexual risk-taking among MSM. • Studies have found a relationship between: • Stressful or traumatic life events (incl. childhood sexual abuse, sexual coercion in adulthood, domestic violence, witnessing the death or physical harm of another person, etc.). • Sexual risk-taking. • Limitations of prior research: • Focused on the objective occurrence of stressful or traumatic events and their effects, but not on a person’s emotional reaction to the events. • Effects have been generally in the modest range.
Specific Aims • The current study assessed psychosocial and behavioral associations of STD and HIV risk behavior among a cohort of Massachusetts MSM screening in for a significant emotional response to a stressful or traumatic life event (i.e., screening in for symptoms of PTSD). • We hypothesized that it is not the event itself, but one’s emotional response to it that may differentiate MSM who engage in HIV/STD risk behavior from those who do not.
Methods Participants and Procedures • Between March 2006 and May 2007, 189 participants completed a quantitative survey (approx 1 hour in duration). • Participants were eligible if they were: • 18 years of age or older. • A Massachusetts resident. • Self-reported having sex with men. • Recruitment: • Convenience sample (n = 63). • Modified RDS sample (n = 126). • All study measures and procedures were IRB-approved by The Fenway Institute. • Supported by the Massachusetts Department of Public Health.
Methods Predictors of Interest • Experiencing a worst event • Asked participants an open-ended question about worst event ever experienced. • Responses were dichotomized. • Significant emotional response to a worst event • SPAN (Startle, Physiological arousal, Anger, and Numbness) (Meltzer-Brody et al., 1999). • Score 6 or greater indicated a significant emotional reaction to the worst event (i.e., PTSD symptomatology).
Methods Outcome Variables • Unprotected anal sex (either insertive or receptive) in the past 12 months. • CES-D: Center for Epidemiologic Studies Depression Scale (DHHS, 2004; Hann et al., 1999; Radloff, 1977). • SPIN: Symptoms of social anxiety (psychometric properties of the Social Phobia Inventory) (Connor et al., 2000). • CAGE: Screening instrument for alcoholism (Ewing, 1984; Knowlton et al., 1994; Mayfield et al., 1974).
Methods • Data analysis • SAS version 9.1 (Cary, NC) statistical software; statistical significance at the p<0.05 level. • Comparisons between MSM screening in for a significant emotional response (SPAN 6+) and those not screening in (SPAN 0-5). • Descriptive statistics,Chi-square and t-test statistics. • Bivariate and multivariable logistic regression. • Variables that were statistically significant in bivariate regression analyses were retained in final multivariable logistic regression models. • Controlled for race, sexual orientation, and HIV status.
Results: Demographics Race/Ethnicity: Sexual Orientation:
Results: Demographic comparisons • 93% of the sample (n=176) reported having experienced a worst event. • 60% of the sample (n=113) screened in for a significant emotional response to a stressful or traumatic life event (PTSD symptomatology, SPAN score 6+). • Men screening in for a significant emotional response were more likely to: • Be white (OR=1.93; p<0.03). • Be gay-identified (OR=2.01; p<0.03).
Results: Risk behavior in past 12 months Substance use during sex in past 12 months
Results: Significant emotional response in relation to unprotected anal sex in past 12 months
Results: Significant emotional response in relation to depression and social anxiety
Limitations • Emotional response to a stressful or traumatic life event was assessed using a PTSD screener (e.g., did not measure intensity of more remote events, or duration or frequency of events). • Data is constrained by methodological difficulties present in most stressful life event research (namely inconsistencies conceptualizing and measuring stressful/traumatic events). • RDS led to diverse sample but incentives may have resulted in more socially marginalized group of MSM (i.e., prevalence of stressful/traumatic events may not be generalizable across all MSM). • Since one third of participants were patients at Fenway, a community health center specializing in LGBT healthcare, the sample may be more gay-identified with a higher prevalence of HIV infection/STD history than the greater Boston area MSM population.
Discussion • Experiencing a stressful or traumatic life event did not in and of itself predict increased sexual risk-taking or co-morbid psychosocial health problems. • However, currently having a significant emotional response to a stressful or traumatic life event (PTSD symptomatology) did predict unprotected anal sex in the past 12 months, depression, and social anxiety. • Findings suggest that having a significant emotional response to a stressful or traumatic life event is predictive of sexual risk-taking over and above the effects of the event itself. • The current study can be placed in the context of other research documenting elevated rates of co-occurring psychosocial issues facing high-risk MSM. • Potential benefit of incorporating how to cope with these issues in HIV prevention and care interventions.