Download
1 / 27
290 likes | 442 Vues
Is it time for new standards in the management of gastric cancer?. Professor Yoon-Koo Kang U niversity of Ulsan College of Medicine, Asan Medical Center Seoul, Korea. Case study: initial presentation. Gastroscopy large ulceroinfiltrative lesion encircling the antral lumen Biopsy

E N D
Is it time for new standards in themanagement of gastric cancer? Professor Yoon-Koo KangUniversity of Ulsan College of Medicine, Asan Medical CenterSeoul, Korea
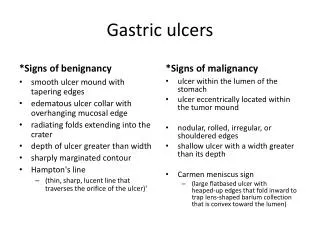
Case study: initial presentation • Gastroscopy • large ulceroinfiltrative lesion encircling the antral lumen • Biopsy • tubular adenocarcinoma, M/D
What would you recommend? • Best supportive care alone • XP (Xeloda + cisplatin q3w) • 5-FU + cisplatin • DCF (docetaxel + cisplatin + 5-FU q3w) • ECF (epirubicin + cisplatin + 5-FU q3w) • FOLFIRI (5-FU + leucovorin + irinotecan q1w) • DCX (docetaxel + cisplatin + Xeloda q3w)
What would you recommend? • Best supportive care alone • XP (Xeloda + cisplatin q3w) • 5-FU + cisplatin • DCF (docetaxel + cisplatin + 5-FU q3w) • ECF (epirubicin + cisplatin + 5-FU q3w) • FOLFIRI (5-FU + leucovorin + irinotecan q1w) • DCX (docetaxel + cisplatin + Xeloda q3w)
Patient enrolled in the internationalXP vs FP ML17032 trial RANDO MIS ATION XP Xeloda 1000mg/m2 bid d114 cisplatin 80mg/m2 d1 q3w n=156 Advanced and/ormetastaticgastric cancer n=316 FP 5-FU ci 800mg/m2 d15 cisplatin 80mg/m2 d1 q3w n=160 • Primary endpoint: non-inferiority in PFS Kang Y-K et al. Ann Oncol 2006;17(Suppl. 6):vi19 (Abst O-003)
Rationale for study • FP/CF is a reference regimen for AGC • Xeloda monotherapy is effective and well tolerated in AGC1–4 • XP in Phase II5 • ORR: 55% • TTP: 5.8 months • good safety 1. Hong YS et al. Ann Oncol 2004;15:1344–72. Leon-Rodriguez E et al. Ann Oncol 2002;13(Suppl. 5):191 (Abst 708)3. Sakamoto J et al. Anticancer Drugs 2006;17:231–64. Koizumi W et al. Oncology 2003;64:232–65. Kim TW et al. Ann Oncol 2002;13:1893–8
Case study: XP chemotherapy 22 August 2004 Before treatment After cycle 2 • PR 01 October 2004
Case study: XP chemotherapy 10 November 2004 After cycle 4 • cPR After cycle 8 • CR? 07 February 2005
Case study:carcinoembryonic antigen (CEA) levels CEA (ng/mL) Upper normal limit August 04 October 04 January 05 February 05 December 04 November 04 September 04
0 2 4 6 8 10 12 14 16 18 20 22 24 26 Months ML17032 trial:primary endpoint met – PFS HR=0.81 Estimated probability 1.0 XP (n=139) FP (n=137) 0.8 0.6 HR=0.81 (95% CI: 0.63–1.04) Compared to HR upper limit 1.25, p=0.0008 0.4 0.2 5.0 5.6 0.0 Per protocol Kang Y-K et al. Ann Oncol 2006;17(Suppl. 6):vi19 (Abst O-003)
PFS: robust results in subgroups Favours XP Favours FP Per protocol population Prior chemotherapyNo prior chemotherapy MaleFemale ≤65 years >65 years KPS <80%KPS 80% 1 metastatic site 2 metastatic sites 276 28248 185 91 238 38 30246 98178 0.2 0.6 1.0 1.4 1.8 2.2 2.6 HR ( 95% CI) Kang Y-K et al. Ann Oncol 2006;17(Suppl. 6):vi19 (Abst O-003)
XP vs FP: non-inferior OS – HR=0.85 Estimated probability 1.0 XP (n=139) FP (n=137) 0.8 0.6 HR=0.85 (95% CI: 0.64–1.13) Compared to HR upper limit 1.25, p=0.0076 0.4 0.2 9.3 10.5 0.0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 Months Per protocol Kang Y-K et al. Ann Oncol 2006;17(Suppl. 6):vi19 (Abst O-003)
Multivariate analysis demonstrates robustness of results • Region-stratified factors considered sex, ageprior chemotherapy, Karnofsky score, bone metastases, metastatic sites and serum bilirubin Intent-to-treat Kang Y-K et al. Proc ESMO 2006 (Abst O-003)
Superior response rate with XP Intent-to-treat, investigators’ assessment Kang Y-K et al. Ann Oncol 2006;17(Suppl. 6):vi19 (Abst O-003)
XP vs FP: comparable toxicities Patients (%) Grade 3/4 AEs XP (n=156) FP (n=155) HFS Nausea/vomiting Diarrhoea Stomatitis Febrileneutropenia Leucopenia Neutropenia Kang Y et al. Ann Oncol 2006;17(Suppl. 6):vi19 (Abst O-003)
Experience of first-line XP chemotherapy at AMC: March 2000 – December 2004 *p<0.05, among subgroups Lee SS et al. Jpn J Clin Oncol 2007;37:30–7
Experience of first-line XP chemotherapy at AMC: March 2000 – December 2004 *p<0.05, among subgroups Lee SS et al. Jpn J Clin Oncol 2007;37:30–7
Experience of first-line XP chemotherapy at AMC: March 2000 – December 2004 *p<0.05, among subgroups • Disease status (tumour burden) and PS were independent prognostic factors Lee SS et al. Jpn J Clin Oncol 2007;37:30–7
XP is safe in a clinical practice setting Lee SS et al. Jpn J Clin Oncol 2007;37:30–7
Case study: XP chemotherapy Before treatment After cycle 7 • Biopsy: no cancer
What would you recommend? • Stop treatment and follow-up only • Change chemotherapy regimen and continue • Exploratory laparotomy and resection of residual diseases
Remission for 9 monthswithout chemotherapy • Stopped chemotherapy since February 2005 • Follow-up every 3 months • abdomen and pelvis CT • GFS • CEA
Salvage chemotherapy • Docetaxel 75mg/m2 d1 q3w • 6 cycles: SD • Irinotecan 350mg/m2 d1 q3w • 4 cycles: SD • FOLFOX q2w • 12 cycles: SD
25 January 2007:patient with PD, alive without treatment CEA: 20.9ng/mL
XP: a potential new standardchemotherapy in AGC • As effective as 5-FU/cisplatin • Improved tolerability • Avoids inconvenience and complicationsassociated with infused 5-FU Xeloda should be the backbone ofnew standards in AGC