Download
1 / 48
510 likes | 879 Vues
Structure, Growth, and Mineralization of Bone. Lecture 4. Case study: A young man was of average height till he was 15 years of age, but he was still growing at 24 years. He was 6ft. 7inches tall, but his bone were weak. What do you think was the problem?.

E N D
Case study: A young man was of average height till he was 15 years of age, but he was still growing at 24 years. He was 6ft. 7inches tall, but his bone were weak. What do you think was the problem?
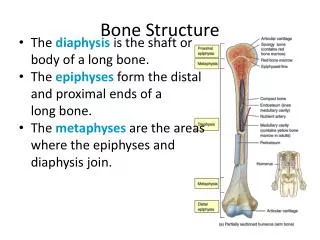
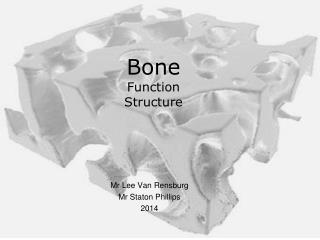
Bone is a specialized connective tissue that, along with cartilage, forms the skeletal system • The role of bone • Bone has a protective and supportive role. • It is metabolically active, and stores many minerals • It provide defense against acidosis • It forms a trap for some dangerous minerals such as lead
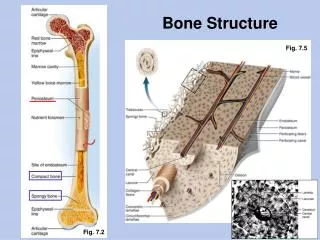
Bone • Compact (cortical)Not completely solid, but permeated by Haversian canals containing blood vessels and bone cells. • Cancellous (trabecular)Honey comb network of calcified tissue on the inner side. The terms cortical and cancellous describe the gross arrangement of bone tissue. In general bones are compact on the outside and cancellous (spongy) on the inside. Microscopically bone is composed of cells and extracellular matrix
Since the surface to volume ratio of cancellous bone is so large it has an important role to play in calcium ion homeostasis (the importance of cancellous bone in Calcium homeostasis is exemplified by the fact that 99% of the total body Calcium is stored within the skeleton).
A scanning electron image (B) that shows bone collagen fibrils in both longitudinal and cross sections. The back-scattered electron image (C) shows the regular patterns of collagen in layers in bone, which is why normal bone is called lamellar bone.Images from Marian Young
Biochemical functions of bone cells • Osteoblasts: • Synthesize webs of collagen fibers, proteoglycans and glycoproteins. • Control bone mineralization. • Osteocytes: • May contribute to the maintenance of calcium homeostasis , • May have a role in activating bone turnover. • Osteoclasts: • They act in bone resorption and the release of calcium and phosphate into the plasma. • Osteoclasts are able to resorb bone by selectively producing an extremely low pH within the immediate micro-environment of their action by carbonic anhydrase II
Osteoprogenitor cells • These are functionally undifferentiated mesenchymal cells • Under the appropriate stimulation these cells may differentiate into functional osteoblasts. • Lining cells • Are former osteoblasts which have become flat and pancake-shaped, lining the entire surface of the bone. • Are responsible for immediate release of calcium from the bone if the blood calcium is too low. • Protect the bone from chemicals in the blood which dissolve crystals (such as pyrophosphate). • Have receptors for hormones and factors that initiate bone remodeling.
Bone consists of mineral salts (mainly calcium phosphate, approximately 60% of weight) deposited on an organic matrix. • Water comprises approximately 25% of adult bone mass.
Bone matrix • The matrix, which is formed before the mineral is deposited, and can be considered the scaffolding for the bone • It consists of proteins, of which collagen type I is the most important, proteoglycans, and a smaller fraction of lipids and water.
Figure 3: Main features of the collagen molecule and its relation to the structure of the fibril
Osteogenesis Imperfecta • Osteogenesis imperfecta (OI and sometimes known as Brittle Bone Disease, or "Lobstein syndrome") is a genetic bone disorder. People with OI are born without the proper protein (collagen), or the ability to make it, usually because of a deficiency of Type-I collagen.
Bone matrix: non-collagen, calcium binding proteins • They are negatively charged glycoproteins • Therefore, they have a high calcium binding potential and are implicated in bone calcification • They include Osteopontin, Osteonectin, Osteocalcin, Matrix extracellular protein, Bone sialoprotein
Osteopontin (RMM 32 600 kD): • Rich in aspartic acid + some sialic acid. • Synthesis is stimulated by vitamin D. • Bind hydroxyapatite. • Associated with the attachment of osteoclasts to the matrix. • Binds to integrins • Increases angiogenesis (makes new blood vessels) which enhances bone resorption in some situations
Osteonectin (RMM 35 000 kD): • Binds collagen and hydroxyapatite. • Also referred to as "Bone connector“, and may regulate mineralization • Its synthesis is associated with bone formation and remodeling.
Osteocalcin(MW 11 000): • The smallest MW. • Contains γ-carboxyglutamic acid (2 or 3 residues) • Binds to hydroxyapatite (may regulate crystal size) • Its synthesis is stimulated by vitamin D. • Vitamin K is needed for the carboxylation of glutamic acid. • Used as a marker of bone metabolism, as its production and levels in the blood reflect osteoblastic activity.
Matrix Gla protein (MW 12 000): • Contain γ-carboxyglutamic acid. • Second smallest MW. • Synthesis is stimulated by vitamin D & require vitamin K. • Function is not clear, but it appears to inhibit mineralization
Bone Sialoprotein: • Rich in sialic acid. • Binds to integrins, may assist cancer cells • No clear function.
Fibronectin • Relatively abundant • May help regulate osteoblast differentiation
Types of bone matrix • Woven bone: • Collagen fibrils are distributed within the matrix in a haphazard arrangement. • It is rapidly formed however it is mechanically weak. • It is the first bone matrix formed during skeletal growth and development and healing. • The presence of woven bone in the context of mature skeleton is abnormal but non-specific. • Lamellar bone: • Collagen fibrils have an ordered arrangement in “curving linear arrays”. • This is a mechanically much more sound matrix. • It is the type of bone found in the mature skeleton.
Bone Minerals • Bone mineral is so closely associated with the organic matrix, especially with the collagen component. It consists of: • 19-26% Calcium (Ca2+) • 9-12% Phosphate (Po43-) • 2-4 % Carbonate (Co32-) • 0.2- 0.3 % Magnesium (Mg2+) • Bone also contain Na and some other minerals in small amounts
The mineral is composed of narrow crystallites in the form of long cylinders; about 5 nm wide (60-70 nm in length), arranged parallel to the collagen fibers. Some cylinders aggregate to from thicker structures approximately 20 nm wide. • The crystal structure is similar to, but not identical with naturally occurring hydroxyapatite [Ca10 (PO4)6 (OH)2 ]. Bone mineral has a higher content of carbonate and some phosphate may be replaced by sulphate or silicates.
BONE FORMATION AND GROWTH • Bone Formation:occurs by the coordinated activity of: chondrocytes, osteoclasts and osteoblasts Undifferentiated mesenchymal cells Transforming growth factors (TGFs), other growth factors, chondrogenic stimulating activity (CSA), steroid and peptide hormones and collagens & other extracellular matrix proteins A- Chondrogenic line (cartilage forming) Chondrocytes + osteoblasts B- Osteogenic line (bone forming) Osteoblasts
Osteoblasts Osteoclasts Bone formation by Endochondral ossification (cartilage is first formed and later replaced by bone) (most of the skeleton) A- Chondrogenic line (cartilage forming) Chondrocytes and osteoblasts • A rod of Cartilage is formed by chondrocytes • Osteoid tissue is formsd by osteoblasts outside the cartilage rod • (Osteoid formation, Mineralization, Vascularization)10-15 • Osteoblasts become embeded in osteoid & mature osteocytes • Cartilage rod (center) bone marrow • Cartilage bone Growth stops when all cartilage (except at the articular surface of the joint) is replaced by bone, and the epiphyses close. (Mineralization + vascularization)
Case study: A young man was of average height till he was 15 years of age, but he was still growing at 24 years. He was 6ft. 7inches tall, but his bone were weak. What do you think was the problem? • Many factors play a role in controlling growth of bone including certain hormones, local mediators and nutritional status
Factors affecting formation & growth of bone • Pitutary gland: • Hypopituitarism → reduced rate of skeletal growth • Growth hormone: • Important until epiphesial closure. • Acts by: • influencing IGF-1 (regulate IGF-1 production) • stimulation of cell division (prechondrocytes + osteoblasts)
Thyroid hormone: • May stimulate chondrocyte maturation. • Sex hormones: • Oestrogen help regulate the rates of bone formation and bone resorption. • It inhibits osteoclasts and their precursors. • It is also required for the process of epiphyseal closure in both sexes and testosterone additionally in males. • Glucocorticoids
Hormonal Abnormalities • Oversecretion of hGH during childhood produces giantism • Undersecretion of hGH or thyroid hormone during childhood produces short stature • Both men or women that lack oestrogen receptors on cells, or are unable to convert testosterone into oestrogen grow taller than normal (the case mentioned earlier) • oestrogen is responsible for closure of growth plate
Local mediators (regulators) • Bone cells produce molecules (usually proteins) that communicate with other cells. • They act on nearby cells, and thus are considered local regulators. • These factors control cell division (proliferation) • One important pair are Indian hedgehog and PTHrp
A mutation causing a constant activation of PTH receptor causes short stature and other signs of hyperparathyroidism, but with low serum level (Jansen’s chondrodysplasia) • Another mutation causing inactive receptor can be fatal in the foetus, or the bones fail to elongate (Blomstrand chondrodysplasia) • More information can be found at: http://depts.washington.edu/bonebio/ASBMRed/growth.html
Blomstrand chondrodysplasia Jansen’s chondrodysplasia
Examples of Local mediators: Example 1: fibroblast growth factors. A mutation affecting FGF Receptor-3 leads to achondroplasia, the commonest cause of human short stature.
Achondroplasia. This picture shows twin brothers. The twin on the right has achondroplasia.
Example 2: Transcription factors, controlling the formation of mRNAs. Mutations in TF msx1 & msx2 leads to abnormalities in craniofacial development.
Growth factors • Bone morphogenetic proteins (BMPs): • BMPs are produced in the bone or bone marrow. • They bind to BMP receptors that are on mesenchymal stem cells within the bone marrow. • This causes the cells to produce Cbfa 1, which is a factor that activates the DNA so proteins can be made • When Cbfa 1 activates the genes, the cells differentiate into mature osteoblasts. • Without Cbfa 1, the cells would turn into fat cells instead.
Insulin-like growth factors (IGFs): • These growth factors are produced by osteoblastic cells in response to several bone active hormones, such as parathyroid hormone and estrogens, or BMPs. • IGFs accumulate in the bone matrix and are released during the process of bone remodeling by osteoclasts. • IGFs stimulate osteoblastic cell replication -- in other words, they cause the osteoblasts to divide, forming new cells. They may also induce differentiation.
Cytokines • Interleukin-1 (IL-1), interleukin-6 (IL-6), and tumor necrosis factor (TNF) family of cytokines • These factors are produced by osteoblastic cells in response to systemic hormones or other cytokines. • IL-6 can cause: • Bone marrow stem cells to differentiate into pre-osteoclasts • Changes in proliferation and differentiation of osteoblasts • Inhibition of apoptosis of osteoblasts
Dietary Factors: • Calcium, phosphate, vitamins D, A and C are most important for endochondrial ossification. • Also important (but less) are: zinc, magnesium and vitamin K. • More recently researchers investigated the effects of moderate magnesium (Mg)-restricted diet on bone formation and bone resorption in rats. Mg-restricted diet induced a decrease in bone formation and an increase in bone resorption. • Restriction of energy intake also effects bone formation.
MINERLIZATION OF BONE • Nucleation agent theory: • Non-collagenous proteins of the matrix provide 'nucleation' sites of the correct geometry for deposition of calcium phosphate. • Note: • Calcium phosphate is relatively insoluble in water and precipitation of this salt can occur spontaneously if the concentrations of calcium, phosphate, or both, cause the 'solubility product' of calcium phosphate to be exceeded • The solubility product for calcium phosphate is:Ksp = [Ca2+]3[PO43-]2 • It is pH dependent, and at pH 7.0 its value is 25.
‘Matrix vesicles’ theory: • Osteoblasts and chondrocytes acquire calcium and phosphate ions, form concentrated calcium phosphate at the cell periphery and exfoliate it as vesicles (which also contain alkaline phosphate) prior to its deposition on collagen, and other proteoglycans secreted by osteoblasts
Both theories need enough calcium and phosphate. • Calcium and phosphate ion concentrations in the aqueous medium may be altered by binding to proteins, • Complex localized concentration changes may occur as a result of metabolic processes. • Furthermore, the 'micro-environmental' concentrations of calcium and phosphate in biological systems may not be identical to those in the bulk of the solution.
The structural strength (and therefore its mechanical function) of any bone is determined by the following parameters: • The volume of bone matrix • The type of bone matrix (woven or lamellar, ) • The degree of mineralization of the matrix • The structural arrangement of the matrix • Alterations in any of these parameters will result in a potentially mechanically dysfunctional skeleton.