Mechanical Ventilatior
Mechanical Ventilatior. Outline:. Definition. Indications. Types of ventilators. Ventilator settings. Modes of ventilation. Risks. Weaning . Nursing care for ventilated patient. Mechanical Ventilator.

Mechanical Ventilatior
E N D
Presentation Transcript
Outline: • Definition. • Indications. • Types of ventilators. • Ventilator settings. • Modes of ventilation. • Risks. • Weaning . • Nursing care for ventilated patient.
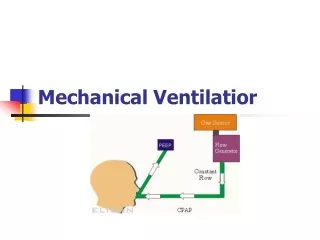
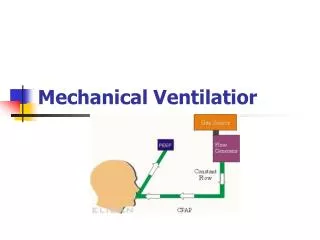
Mechanical Ventilator • A mechanical ventilator is a machine that makes it easier for patients to breathe until they are able to breathe completely on their own. Sometimes the machine is called just a ventilator, respirator or breathing machine. Usually, a patient is connected to the ventilator through a tube (called an endotracheal tube) that is placed in the windpipe.
Indications • Physiologic reasons: include supporting cardiopulmonary gas exchange (alveolar ventilation &arterial oxygenation) and reducing work breathing , e.g pulmonary oedema , pnemonia.
Clinical reasons include reversing hypoxia &Acute respiratory acidosis • Acute respiratory acidosis with partial pressure of carbon dioxide (pCO2) > 50 mmHg and pH < 7.25
Indications which may be due to paralysis of the diaphragm due to Guillain-Barré syndrome, Myasthenia Gravis, spinal cord injury, or the effect of anaesthetic and muscle relaxant drugs • Increased work of breathing as evidenced by significant tachypnea, retractions, and other physical signs of respiratory distress • Hypoxemia with arterial partial pressure of oxygen (PaO2) with supplemental fraction of inspired oxygen (FiO2) < 55mm Hg • Hypotension including sepsis, shock, congestive heart failure
Initial ventilator settings • tidal volume is calculated in milliliters per kilogram. Traditionally 10 ml/kg was used but has been shown to cause barotrauma, or injury to the lung by overextension, so 6 to 8 ml/kg is now common practice in ICU. Hence a patient weighing 70kg would get a TV of 420–480 ml.
Initial ventilator settings • Initial FiO2 • The FiO2 stands for fraction of inspired oxygen, which means the percent of oxygen in each breath that is inspired. (Note that normal room air has ~21% oxygen content). In adult patients who can tolerate higher levels of oxygen for a period of time, the initial FiO2 may be set at 100% until arterial blood gases can document adequate oxygenation.
Initial ventilator settings • Positive end-expiratory pressure (PEEP) It’s applying positive pressure at end of expiration ,used with CV, A/C and SIMV. It aims to prevent alveolar collapse & Increase the surface of gas exchange.
Initial ventilator settings • Respiratory Rate: number of breaths the ventilator delivers per minute. usual setting rate is 4-20breath/min. • Sensitivity: determine the amount of effort the patient must generate to initiate ventilator breath.
Modes of ventilation • Controlled Mechanical Ventilation (CMV). In this mode the ventilator provides a mechanical breath on a preset timing. Patient respiratory efforts are ignored. This is generally uncomfortable for children and adults who are conscious and is usually only used in an unconscious patient. It may also be used in infants who often quickly adapt their breathing pattern to the ventilator timing.
Modes of ventilation • Synchronized Intermittent Mandatory Ventilation (SIMV). In this mode the ventilator provides a pre-set mechanical breath (pressure or volume limited) every specified number of seconds Within that cycle time the ventilator waits for the patient to initiate a breath using either a pressure or flow sensor. When the ventilator senses the first patient breathing attempt within the cycle, it delivers the preset ventilator breath. If the patient fails to initiate a breath, the ventilator delivers a mechanical breath at the end of the breath cycle.
Modes of ventilation • Assist Control (A/C( or continuous mandatory ventilation : deliver gas at preset tidal volume in response to patient’s inspiratory efforts & will initiate breath if patient fails to do so within preset time.
Modes of ventilation • Continuous Positive Airway Pressure(CPAP). • A continuous level of elevated pressure is provided through the patient circuit to maintain adequate oxygenation, decrease the work of breathing, and decrease the work of the heart (such as in left-sided heart failure — CHF). Note that no cycling of ventilator pressures occurs and the patient must initiate all breaths. In addition, no additional pressure above the CPAP pressure is provided during those breaths. CPAP may be used invasively through an endotracheal tube or tracheostomy or non-invasively with a face mask or nasal prongs.
Risks: • Infections - The endotracheal tube in the windpipe makes it easier for bacteria to get into the lungs. As a result, the lungs develop an infection, which is called pneumonia. The risk of pneumonia is about 1% for each day spent on the ventilator. Pneumonia can often be treated with antibiotics. Sometimes the pneumonia can be severe or difficult to treat because of resistant bacteria
Risks: • Collapsed Lung - This is called a pneumothorax. The mechanical ventilator pushes air into the lungs. It is possible for a part of the lung to get over-expanded which can injure it. Air sacs may leak air into the chest cavity and cause the lung to collapse. If this air leak happens, doctors can place a tube in the chest between the ribs to drain out the air leaking from the lung.
Risks: • Lung damage - When the lungs are diseased and not functioning well, they are at greater risk of injury. The pressure to put air into the lungs with a ventilator can be hard on the lungs.
Risks: • Side Effects of Medications - Patients may be given medications, called sedatives, to make them more comfortable while the ventilator pushes air in and out of the lungs. These medications make patients sleepy and help them forget unpleasant experiences. The medications can build up in the body and the patient may remain in a deep sleep for hours to days, even after the medicine is stopped.
Weaning • Is the process of withdrawing the patient from dependence on the ventilator. • Begin during the daytime; allow the patient to rest at night and between trails of weaning. • Place the patient in an upright position. • Causes of weaning failure include poor respiratory or cardiac function ,infection, high metabolic demands, poor nutrition and energy stores, and inadequate rest.
Discontinue weaning if: PH<7.3, PCO2>50torrs , PO2< 60torrs. • The patient becomes anxious , fatigued. • Arrhythmias , homodynamic deterioration.
Care of ventilated patient • Provide care for patient’s artificial airway as needed. • Assess the patient’s peripheral circulation for decreased cardiac output. • Be sure that ventilator alarms are on at all times . • Unless contra indicated turn the patient from side to side every 2hours to facilitate lung expansion. • Place the call light within the patient’sreach. • Administer a sedative to relax the patient. • Covering and lubricating eyes. • Provide emotional support.