STDs
STDs. Valerie Robinson D.O. Prevention. Abstinence Risk reduction Vaccines Male or female condoms Cervical diaphragm might protect against cervical GC, CT, trichomonas Male circumcision reduces transmission of herpes, HPV and HIV in heterosexual men

STDs
E N D
Presentation Transcript
STDs Valerie Robinson D.O.
Prevention • Abstinence • Risk reduction • Vaccines • Male or female condoms • Cervical diaphragm might protect against cervical GC, CT, trichomonas • Male circumcision reduces transmission of herpes, HPV and HIV in heterosexual men • Antiretroviral therapy in HIV-infected people • Trichomoniasis, chlamydia, gonorrhea, and syphilis are curable
Screening • Pregnant women should be screened for GC, CT, syphilis, HIV, hepatitis B. Not trich or hep C • Adolescents: Discuss sexual behavior • Screen CT, GC in females <25 • Discuss HIV screen with sexually active or IV drug-using adolescents • MSM: annual screen for HIV, syphilis, oral, anal, and penile gonorrhea and chlamydia • Anyone who has an STD should be screened for HIV
Chlamydia • Chlamydia trachomatis • The most commonly reported STD • CDC recommends yearly chlamydia testing of all sexually active women age 25 or younger, women with risk factors, and all pregnant women. • Symptoms occur 1-3 weeks after exposure • May be transmitted to baby during vaginal delivery, causing conjunctivitis or pneumonia, NOT transmitted through placenta • In pregnant women, there is some evidence that untreated chlamydial infections can lead to premature delivery • Complications: PID, infertility, ectopic, Reiter's syndrome • 10-15% of untreated women progress to PID • Reiter's syndrome : Rare. arthritis, uveitis, conjunctivitis, circinatebalanitis urethritis, cervicitis, Achilles enthesitis,
Chlamydia - Symptoms • Vaginal discharge, UTI • May cause lower abdominal pain, low back pain, nausea, fever, pain during intercourse, or bleeding between menstrual periods, especially if it has progressed to PID. • Men: penile discharge “the clap”, UTI, burning or itching around meatus. Rarely epididymitis: pain, fever, and, rarely, sterility • Rectal: rectal pain, discharge, or bleeding • May be oral • May cause lymphogranulomavenereum
Chlamydia - Diagnosis • Nucleic Acid Amplification Testing (NAAT) Urine • Vaginal swab culture • Infants: conjunctival swab - direct fluorescence antibody [DFA] tests, ELISA, and NAAT
Chlamydia - Treatment • Azithromycin 1 g orally in a single dose • Doxycycline 100 mg orally twice a day for 7 days • Erythromycin base 500 mg orally four times a day for 7 days • Levofloxacin 500 mg orally once daily for 7 days • Infant conjunctivitis OR pneumonia: • Erythromycin base or ethylsuccinate50 mg/kg/day orally divided into 4 doses daily for 14 days • Lymphogranulomavenereum • Doxycycline 100 mg orally twice a day for 21 days • Erythromycin base 500 mg orally four times a day for 21 days (Use this in pregnancy)
Gonorrhea • Very common • Often co-infection with chlamydia • Babies have ocular prophylaxis with erythromycin ointment or silver nitrateOpthalmianeonatorum • May cause PID, infertility, ectopic, epididymitis • PID: abdominal pain and fever. Can lead to internal abscesses and chronic pelvic pain • Diagnosis: urine NAAT, vaginal, or urethral culture, nucleic acid hybridization tests
Gonorrhea - Symptoms • Women: dysuria, increased vaginal discharge, or vaginal bleeding between periods. • Men: dysuria, or a white, yellow, or green penile discharge that usually appears 1 to 14 days after infection. Sometimes men with gonorrhea get painful or swollen testicles • Rectal: discharge, anal itching, soreness, bleeding, or painful bowel movements OR asymptomatic • Oral: sore throat, but usually asymptomatic • Disseminated Gonococcal Infection: petechial or pustularacral skin lesions, asymmetrical arthralgia, tenosynovitis, or septic arthritis. The infection is complicated occasionally by perihepatitis and rarely by endocarditis or meningitis
Gonorrhea - Treatment • #1: combination therapy • ceftriaxone 250 mg IM AND azithromycin 1 g orally single dose OR doxycycline 100 mg orally twice daily for 7 days • CDC no longer recommends cefixime at any dose as a first-line d/t resistance • Alternate: • azithromycin 2 g orally in a single dose • cefixime 400 mg orally AND azithromycin 1 g orally OR doxycycline 100 mg twice daily orally for 7 days • DIG • Ceftriaxone 1 g IM or IV every 24 hours until 24 hours after improvement THEN Oral therapy x 1 week • Children • Uncomplicated: Ceftriaxone 125 mg IM in a single dose • Complicated: Ceftriaxone 50 mg/kg (maximum dose: 1 g) IM or IV in a single dose daily for 7 days
Syphilis • Treponemapallidum • Can have vertical transmission – congenital syphilis • Has 5 stages (primary, secondary, tertiary, latent, and late)
Syphilis – Symptoms • Primary stage: Single or multiple painless chancres lasting 3-6 weeks. May appear up to 3 months after initial infection. • Secondary stage: Rash, may appear on palms and soles • fever, swollen lymph glands, sore throat, patchy hair loss, headaches, weight loss, muscle aches, and fatigue. • Tertiary stage: cardiac or gummatous lesions • Latent stage: may last for years without sx • Late stage: • Occurs in about 15% of untreated people • May appear 10-20 years after initial infection • damage the internal organs, including the brain, nerves, eyes, heart, blood vessels, liver, bones, and joints. Includes neurosyphilis. This damage may be serious enough to cause death.
Syphilis - Complications • Pregnancy – can cause stillbirth • Congenital syphilis - developmental delay, seizures, or death. • Neurosyphilis – can occur at any stage • cranial nerve dysfunction, meningitis, stroke, acute or chronic altered mental status, loss of vibration sense, and auditory or neuroretinitis, optic neuritis • Jarisch-Herxheimer reaction is an acute febrile reaction frequently accompanied by headache, myalgia, fever, and other symptoms that usually occur within the first 24 hours after the initiation of any therapy for syphilis
Syphilis - Diagnosis • Dark field microscopy=definitive • Spirochetes • Nontreponemal • VRDL (Venereal Disease Research Laboratory) • RPR (Rapid plasma reagin) • May have false positive d/t autoimmune dz • Treponemal • Fluorescent Treponemal Antibody Absorbed test [FTA-ABS] • T. pallidum passive particle agglutination [TP-PA] assay • ELISA • chemiluminescence immunoassays
Syphilis - Treatment • Primary and Secondary and Early Latent • Benzathine penicillin G 2.4 million units IM in a single dose • Infants and children: Benzathine penicillin G 50,000 units/kg • Tertiary • Benzathine penicillin G 7.2 million units total, administered as 3 doses of 2.4 million units IM each at 1-week intervals • Late Latent • Benzathine penicillin G 7.2 million units total, administered as 3 doses of 2.4 million units IM each at 1-week intervals • Neurosyphilis • Aqueous crystalline penicillin G 18–24 million units per day, administered as 3–4 million units IV every 4 hours or continuous infusion, for 10–14 days • Pregnancy: same as above • Congenital • Aqueous crystalline penicillin G 100,000–150,000 units/kg/day, administered as 50,000 units/kg/dose IV every 12 hours during the first 7 days of life and every 8 hours thereafter for a total of 10 days • Procaine penicillin G 50,000 units/kg/dose IM in a single daily dose for 10 days • If diagnosed later in life: Aqueous crystalline penicillin G 200,000–300,000 units/kg/day IV, administered as 50,000 units/kg every 4–6 hours for 10 days
HIV • Course: brief acute retroviral syndrome that typically transitions to a multiyear chronic and clinically latent illness. • Depletes CD4 lymphocytes • Progresses to AIDS estimated median time of approximately 11 years. AIDS increases life-threatening opportunistic infections. • Most in USA are HIV-1. HIV-2 West Africa, Portugal • They are highly contagious in the first stages of infection.
HIV - Symptoms • fever, malaise, lymphadenopathy, and skin rash Occur within a few weeks of infection • Opportunistic infections.
HIV - Diagnosis • Serologic screening for antibodies to HIV-1, HIV-2 Using ELISA • Confirm Ab with Western Blot, or Indirect immunofluorescence assay (IFA) or virologic test • Virologic testing looks for HIV antigens or RNA • HIV Ab is detected within 3 months of infection • In children <18m, use virology • CD4 T-lymphocyte count and viral load confirms AIDS • New OraQuick swab October 2012
HIV - Pregnancy • 15%–25% of infants born to untreated HIV-infected mothers will become infected with HIV; • an additional 12%–14% of infants born to infected mothers who breastfeed into the second year of life will become infected • risk for perinatal HIV transmission can be reduced to <2% through the use of antiretroviral therapy and and elective cesarean section at 38 weeks of pregnancy and by avoiding breastfeeding
HIV - Treatment • HAART • Zidovudine • Nevirapine
Hepatitis A • Incubation period of approximately 28 days. • Self-limited disease • Fecal-oral transmission • Symptoms compatible with acute viral hepatitis • 10%–15% of patients experience a relapse of symptoms during the 6 months after acute illness • Antibody produced in response to HAV infection persists for life and confers protection against reinfection. • Diagnosis: Serum HepAIgM • Tx: supportive care • Post-exposure prophylaxis in un-vaccinated persons: single-antigen vaccine or IG (0.02 mL/kg)
Hepatitis B • Incubation period 6 weeks-6months • Self-limited or chronic • Diagnosis: Serum IgM anti-HBc, HBs antigen • Treatment: • Acute: supportive care • Chronic: antiviral suppressive therapy • Post-exposure prophylaxis • HepB vaccine, HBIG
Hepatitis C • Mostly asymptomatic • Leads to cirrhosis • Diagnosis: • anti-HCV immunoassay, ELISA, or enhanced chemiluminescenceimunoassay • Reverse Transcriptase Polymerase Chain Reaction(RT-PCR) Used for confirmation • Treatment: Combination therapy with pegylated interferon and ribavirin
Pediculosis Pubis AKA pubic lice AKA “crabs” • Symptoms: itching • Treatment • Permethrin1% cream rinse applied to affected areas and washed off after 10 minutes • Pyrethrinswith piperonylbutoxide applied to the affected area and washed off after 10 minutes • Ivermectin250 μg/kg orally, repeated in 2 week
Chancroid • Hemophilusducreyi • Symptoms: painful genital ulcer and tender suppurative inguinal adenopathy • Diagnosis: culture, R/O syphilis, herpes
Chancroid - Treatment • Azithromycin 1 g orally in a single dose • Ceftriaxone 250 mg intramuscularly (IM) in a single dose • Ciprofloxacin* 500 mg orally twice a day for 3 days* • Erythromycin base 500 mg orally three times a day for 7 days • * Ciprofloxacin is contraindicated for pregnant and lactating women.
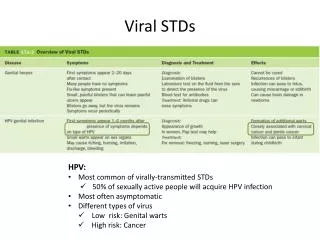
HPV • Most common STD • 40 HPV types that infect human mucosal surfaces • at least 50% of sexually active men and women get it at some point in their lives. • In 90% of cases, the body’s immune system clears HPV naturally within two years. • Genital warts, cervical cancer, cancers of the vulva, vagina, penis, anus, and oropharynx • Gay and bisexual men are about 17 times more likely to develop anal cancer than men who only have sex with women. • Warts don’t become cancer • Usually asymptomatic • Rarely vaginal to baby transmission during birth. HPV types 6 and 11 can cause juvenile onset recurrent respiratory papillomatosis
HPV - Prevention • Cervarix - 16 and 18, which cause 70% of cervical cancers • Gardasil - HPV 16 and 18, as well as HPV 6 and 11, which cause 90% of genital warts • Recommended for girls and boys age 11-26, may begin at age 9. • Series of 3 shots, given at T, T+2months, T+6months • HPV DNA test with Paps • May do anal paps in gay or bisexual men or HIV infected persons • Vaccine should not be given to pregnant women d/t lack of data
HPV - Treatment • Wart • Podofilox0.5% solution or gel (patient-applied) • Imiquimod5% cream (patient-applied) • Sinecatechins15% ointment (patient-applied) • Cryotherapywith liquid nitrogen or cryoprobe. Repeat every 1–2 weeks. • Podophyllinresin 10%–25% in a compound tincture of benzoin • Trichloroaceticacid (TCA) or Bichloroacetic acid (BCA) 80%–90% • Surgical removal either by tangential scissor excision, tangential shave excision, curettage, or electrosurgery. • Imiquimod, sinecatechins, podophyllin, and podofilox should not be used during pregnancy • Treat cervical cancer as per guidelines • Vaccines do NOT treat existing HPV
Herpes • Most genital herpes is caused by HSV-2 • HSV-1 can cause genital herpes, but it more commonly causes infections of the mouth and lips, so-called “fever blisters. • May be transmitted whether or not there is an active outbreak • Occurs in areas not covered by condoms
Herpes - Symptoms • First episode may have fever and lymphadenopathy as well as sores • blisters on or around the genitals or rectum. The blisters break, leaving tender ulcers • Multiple outbreaks occurring weeks or months apart. Often 4-5 per year, decreasing in frequency
Herpes • C/S is performed if a pregnant woman has active lesions at delivery • Diagnosis: wound cx, PCR for DNA, blood antibodies, visual • There is no cure, but suppressive therapy reduces the frequency of genital herpes recurrences by 70%–80% in patients who have frequent recurrences
Herpes - Treatment • First episode • Acyclovir 400 mg orally three times a day for 7–10 days • Acyclovir 200 mg orally five times a day for 7–10 days • Famciclovir250 mg orally three times a day for 7–10 days • Valacyclovir1 g orally twice a day for 7–10 days • *Treatment can be extended if healing is incomplete after 10 days of therapy. • Pregnancy – acyclovir seems to be okay and may be used • Suppression • Acyclovir 400 mg orally twice a day • Famiciclovir250 mg orally twice a day • Valacyclovir500 mg orally once a day* • Valacyclovir1 g orally once a day • * Valacyclovir 500 mg once a day might be less effective than other valacyclovir or acyclovir dosing regimens in patients who have very frequent recurrences (i.e., ≥10 episodes per year).
Herpes - Treatment • Recurrent episodes • Acyclovir 400 mg orally three times a day for 5 days • Acyclovir 800 mg orally twice a day for 5 days • Acyclovir 800 mg orally three times a day for 2 days • Famciclovir125 mg orally twice daily for 5 days • Famciclovir1000 mg orally twice daily for 1 day • Famciclovir500 mg once, followed by 250 mg twice daily for 2 days • Valacyclovir500 mg orally twice a day for 3 days • Valacyclovir1 g orally once a day for 5 days • Severe disease with complications • Acyclovir5–10 mg/kg IV Q8H x 2–7 days or until clinical improvement is observed, followed by oral antiviral therapy to complete at least 10 days of total therapy. • Neonatal herpes • Acyclovir20 mg/kg IV every 8 hours for 21 days for disseminated or CNS • 14 days if only skin and mucous membranes are involved
Trichomonas • Trichomonasvaginalis • About 70% of infected people do not have any signs or symptoms. • Pregnancy Complications: low birth weight, preterm delivery
Trichomonas - Symptoms • May be asymptomatic • Symptoms may not appear until a month after infection or may be intermittent. • Men with trichomoniasis may feel itching or irritation inside the penis, burning after urination or ejaculation, or some discharge from the penis. • Women with trichomoniasis may notice itching, burning, redness or soreness of the genitals, discomfort with urination, or a malodorous discharge that is white, yellowish, or greenish.
Trichomonas - Diagnosis • Wetprep shows trichomonas organisms • OSOM Trichomonas Rapid Test: an immunochromatographiccapillary flow dipstick • Affirm VP III: nucleic acid probe • Culture • NAAT
Trichomonas - Treatment • Metronidazole 2 g orally in a single dose • Tinidazole2 g orally in a single dose • Metronidazole 500 mg orally twice a day for 7 days
Always • Treat the partner • Educate • Vaccinate – Hepatitis A, Hepatitis, B, HPV
References • cdc.gov • “Update to CDC's Sexually Transmitted Diseases Treatment Guidelines, 2010: Oral Cephalosporins No Longer a Recommended Treatment for GonococcalInfections.” Morbidity and Mortality Weekly Report. August 10, 2012 / 61(31);590-594. www.cdc.gov/mmwr • “Sexually Transmitted Diseases Treatment Guidelines, 2010.” Morbidity and Mortality Weekly Report. December 17, 2010 / Vol. 59 / No. RR-12. www.cdc.gov/mmwr