Download
1 / 112
1.18k likes | 1.54k Vues
21. The Immune System: Innate and Adaptive:Body Defenses: Part A. Immunity. Resistance to disease Immune system has two intrinsic systems Innate (nonspecific) defense system Adaptive (specific) defense system. Immunity . Innate defense system has two lines of defense

E N D
21 The Immune System: Innate and Adaptive:Body Defenses: Part A
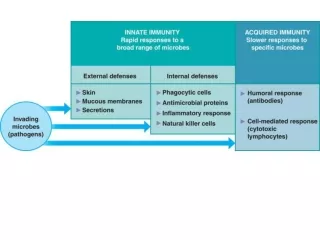
Immunity • Resistance to disease • Immune system has two intrinsic systems • Innate (nonspecific) defense system • Adaptive (specific) defense system
Immunity • Innate defense system has two lines of defense • First line of defense is external body membranes (skin and mucosae) • Second line of defense is antimicrobial proteins, phagocytes, and other cells • Inhibit spread of invaders • Inflammation is its most important mechanism
Immunity • Adaptive defense system • Third line of defense attacks particular foreign substances • Takes longer to react than the innate system • Innate and adaptive defenses are deeply intertwined
Surface barriers • Skin • Mucous membranes Innate defenses Internal defenses • Phagocytes • NK cells • Inflammation • Antimicrobial proteins • Fever Humoral immunity • B cells Adaptive defenses Cellular immunity • T cells Figure 21.1
Innate Defenses • Surface barriers • Skin, mucous membranes, and their secretions • Physical barrier to most microorganisms • Keratin is resistant to weak acids and bases, bacterial enzymes, and toxins • Mucosae provide similar mechanical barriers
Surface Barriers • Protective chemicals inhibit or destroy microorganisms • Skin acidity (pH of 3 – 5) • Lipids in sebum and Dermcidinin eccrine sweat glands • HCl and protein-digesting enzymes of stomach mucosae • Lysozyme of saliva and lacrimal fluid • Mucus
Surface Barriers • Respiratory system modifications • Mucus-coated hairs in the nose • Cilia of upper respiratory tract sweep dust- and bacteria-laden mucus from lower respiratory passages
Internal Defenses: Cells and Chemicals • Necessary if microorganisms invade deeper tissues • Phagocytes • Natural killer (NK) cells • Inflammatory response (macrophages, mast cells, WBCs, and inflammatory chemicals) • Antimicrobial proteins (interferons and complement proteins) • Fever
Phagocytes: Macrophages • Macrophages develop from monocytes to become the chief phagocytic cells • Free macrophages wander through tissue spaces • E.g., alveolar macrophages • Fixed macrophages are permanent residents of some organs • E.g., Kupffer cells (liver) and microglia (brain)
Phagocytes: Neutrophils • Neutrophils • Become phagocytic on encountering infectious material in tissues
Mechanism of Phagocytosis Step 1: Adherence of phagocyte to pathogen • Facilitated by opsonization—coating of pathogen by complement proteins or antibodies • In order to adhere the phagocytic cell must recognize and be able to bind to something on the outside of the organism-generally the carbohydrate. Some organisms cannot be bound to like the pneumococcus unless it is already coated – opsonization.
Innate defenses Internal defenses (a) A macrophage (purple) uses its cytoplasmicextensions to pull spherical bacteria (green) toward it. Scanning electron micrograph (1750x). Figure 21.2a
1 Phagocyte adheres to pathogens or debris. 2 Phagocyte forms pseudopods that eventually engulf the particles forming a phagosome. Phagosome (phagocytic vesicle) Lysosome 3 Lysosome fuses with the phagocytic vesicle, forming a phagolysosome. Acid hydrolase enzymes 4 Lysosomal enzymes digest the particles, leaving a residual body. 5 Exocytosis of the vesicle removes indigestible and residual material. (b) Events of phagocytosis. Figure 21.2b
Mechanism of Phagocytosis • Destruction of pathogens • Acidification and digestion by lysosomal enzymes – Some organisms cannot be destroyed by the lysosome enzymes – like TB – so a granuloma formed. • Respiratory burst • Release of cell-killing free radicals • Activation of additional enzymes – generally by changes in pH (becomes more basic) and osmolarity in the lysosome • Oxidizing chemicals (e.g. H2O2) • Defensins (in neutrophils) – pierce membrane
Respiratory Burst • Respiratory burst (is sometimes called oxidative burst) is the rapid release of reactive oxygen species (superoxide radical and hydrogen peroxide) from different types of cells. • Usually it denotes the release of these chemicals from immune cells, e.g., neutrophils and monocytes, as they come into contact with different bacteria or fungi. • To maximally activate the respiratory burst – T-helper cells stimulate phagocytes • The respiratory burst also increases the pH and osmolarity in the phagolysosome – thus activating other protein-digesting enzymes that digest the invader.
Chronic granulomatous disease • a diverse group of hereditary diseases in which certain cells of the immune system have difficulty forming the reactive oxygen compounds (most importantly, the superoxide radical) used to kill certain ingested pathogens. This leads to the formation of granulomata in many organs. CGD affects about 1 in 200,000 people in the United States, with about 20 new cases diagnosed each year • There are over 410 known possible defects in the PHOX enzyme complex that can lead to chronic granulomatous disease • There are currently no studies detailing the long term outcome of chronic granulomatous disease with modern treatment. Without treatment children often die in the first decade of life.
Granuloma Granuloma is a medical term for a roughly spherical mass of immune cells that forms when the immune system attempts to wall off substances that it perceives as foreign but is unable to eliminate. Such substances include infectious organisms such as and bacteria and fungi as well as other materials such as keratin and suture fragments. A granuloma is therefore a special type of inflammation that can occur in a wide variety of diseases.
Natural Killer (NK) Cells (CD 16 & CD 56) • Large granular lymphocytes - larger lymphocytes with small granules (stained vesicles) • Target cells that lack “self” cell-surface receptors or cells that display wrong MHCI or MICA • NK cell will not attack if a cell’s LY49 receptor is displayed and can be recognized by the NK cell’s MHCI • Secrete perforans and granzyme • Induce apoptosis in cancer cells and virus-infected cells • Secrete potent chemicals that enhance the inflammatory response
Inflammatory Response • Triggered whenever body tissues are injured or infected • Prevents the spread of damaging agents • Disposes of cell debris and pathogens • Sets the stage for repair
Inflammatory Response • Cardinal signs of acute inflammation: • Redness • Heat • Swelling • Pain (And sometimes 5. Impairment of function)
Inflammatory Response • Macrophages and epithelial cells of boundary tissues bear Toll-like receptors (TLRs) • Eleven recognized TLR • TLRs recognize specific classes of infecting microbes – like Salmonella and TB • Activated TLRs trigger the release of cytokines that promote inflammation and attract WBCs
Inflammatory Response • Inflammatory mediators • Histamine (from mast cells and Basophils) • Blood proteins • Kinins, prostaglandins (PGs), leukotrienes, and complement • Singulair is a leukotriene inhibitor • Released by injured tissue, phagocytes, lymphocytes, basophils, and mast cells
Vasodilation and Increased Vascular Permeability • Inflammatory chemicals cause • Dilation of arterioles, resulting in hyperemia • Increased permeability of local capillaries and edema (leakage of exudate) – edema helps with sweep of organisms and chemicals into capillaries of the lymphatics • Exudate contains proteins, clotting factors, and antibodies
Inflammatory Response: Edema • Functions of the surge of exudate • Moves foreign material into lymphatic vessels • Delivers clotting proteins to form a scaffold for repair and to isolate the area – by walling off the infected area • Streptococcus can produce Streptokinase to break down clot and open the walled off area
Anti-inflammatory agents • NSAID – Non-steroidal antiinflammatory drugs – which are anti-prostaglandins • SAID – Steroidal anti-inflammatory drugs – which are natural and synthetic glucocorticoids
NSAID • drugs with analgesic and antipyretic (fever-reducing) effects and which have, in higher doses, anti-inflammatory effects (reducing inflammation). • There are two main types of NSAIDs, nonselective and selective. The terms nonselective and selective refer to different NSAIDs ability to inhibit specific types of cyclooxygenase (COX) enzymes. • Nonselective NSAIDs — Nonselective NSAIDs inhibit both COX-1 and COX-2 enzymes to a similar degree. • Selective NSAIDs — Selective NSAIDs inhibit COX enzymes found at sites of inflammation (COX-2) more than the type that is normally found in the stomach, blood platelets, and blood vessels (COX-1). • Nonselective NSAIDs — Nonselective NSAIDs include commonly available drugs such as aspirin, ibuprofen (Advil®, Motrin®, Nuprin®), and naproxen (Aleve®), as well as some prescription-strength NSAIDs (table 1). • Selective NSAIDs — Selective NSAIDs (also called COX-2 inhibitors) are as effective in relieving pain and inflammation as nonselective NSAIDs and are less likely to cause gastrointestinal injury. Celecoxib (Celebrex®) is the only selective NSAID currently available in the United States. • Selective NSAIDs are sometimes recommended for people who have had a peptic ulcer, gastrointestinal bleeding, or gastrointestinal upset when taking nonselective NSAIDs. Selective NSAIDs have less potential to cause ulcers or gastrointestinal bleeding, but they do not prevent ulcers that develop for other reasons
Nonselective NSAIDs — Nonselective NSAIDs inhibit both COX-1 and COX-2 enzymes to a similar degree. • Selective NSAIDs — Selective NSAIDs inhibit COX enzymes found at sites of inflammation (COX-2) more than the type that is normally found in the stomach, blood platelets, and blood vessels (COX-1).
Nonselective NSAIDs — Nonselective NSAIDs include commonly available drugs such as aspirin, ibuprofen (Advil®, Motrin®, Nuprin®), and naproxen (Aleve®), as well as some prescription-strength NSAIDs • Selective NSAIDs — Selective NSAIDs (also called COX-2 inhibitors) are as effective in relieving pain and inflammation as nonselective NSAIDs and are less likely to cause gastrointestinal injury. Celecoxib (Celebrex®) is the only selective NSAID currently available in the United States.
SAID (Glucocorticoids) • Glucocorticoids influence all types of inflammatory events, no matter their cause. They induce the lipocortin-1 (annexin-1) synthesis, which then binds to cell membranes preventing the phospholipase A2 from coming into contact with its substrate arachidonic acid. This leads to diminished eicosanoid production. The cyclooxygenase (both COX-1 and COX-2) expression is also suppressed, potentiating the effect. • Glucocorticoids also stimulate the lipocortin-1 escaping to the extracellular space, where it binds to the leukocyte membrane receptors and inhibits various inflammatory events: epithelial adhesion, emigration, chemotaxis, phagocytosis, respiratory burst, and the release of various inflammatory mediators (lysosomal enzymes, cytokines, tissue plasminogen activator, chemokines, etc.) from neutrophils, macrophages, and mastocytes.
Beta Defensins • Beta defensins are a family of mammalian defensins. The beta defensins are antimicrobial peptides implicated in the resistance of epithelial surfaces to microbial colonization. • Present in epithelial mucosal cells – and released when the epithelial cells are damaged • Most defensins function by binding to the microbial cell membrane, and, once embedded, forming pore-like membrane defects that allow efflux of essential ions and nutrients. • Alpha defensins are produced by neutrophils
Innate defenses Internal defenses Tissue injury Release of chemical mediators (histamine, complement, kinins, prostaglandins, etc.) Release of leukocytosis- inducing factor Leukocytosis (increased numbers of white blood cells in bloodstream) Vasodilation of arterioles Increased capillary permeability Attract neutrophils, monocytes, and lymphocytes to area (chemotaxis) Leukocytes migrate to injured area Local hyperemia (increased blood flow to area) Capillaries leak fluid (exudate formation) Margination (leukocytes cling to capillary walls) Initial stimulus Physiological response Signs of inflammation Diapedesis (leukocytes pass through capillary walls) Leaked clotting proteins form interstitial clots that wall off area to prevent injury to surrounding tissue Leaked protein-rich fluid in tissue spaces Result Phagocytosis of pathogens and dead tissue cells (by neutrophils, short-term; by macrophages, long-term) Heat Redness Pain Swelling Temporary fibrin patch forms scaffolding for repair Locally increased temperature increases metabolic rate of cells Possible temporary limitation of joint movement Pus may form Area cleared of debris Healing Figure 21.3
Phagocyte Mobilization • Neutrophils, then phagocytes flood to inflamed sites
Phagocyte Mobilization • Steps for phagocyte mobilization • Leukocytosis: release of neutrophils from bone marrow in response to leukocytosis-inducing factors from injured cells • Margination: neutrophils cling to the walls of capillaries in the inflamed area (selectins) • Diapedesis of neutrophils • Chemotaxis: inflammatory chemicals (chemotactic agent) promote positive chemotaxis of neutrophils
Innatedefenses Internaldefenses Inflammatorychemicalsdiffusingfrom theinflamed siteact as chemotacticagents. 4 Chemotaxis.Neutrophilsfollow chemicaltrail. Capillary wall Basementmembrane Endothelium 1 2 3 Leukocytosis.Neutrophils enter bloodfrom bone marrow. Margination.Neutrophils clingto capillary wall. Diapedesis.Neutrophils flatten andsqueeze out of capillaries. Figure 21.4
Innatedefenses Internaldefenses Inflammatorychemicalsdiffusingfrom theinflamed siteact as chemotacticagents. Capillary wall Basementmembrane Endothelium 1 Leukocytosis.Neutrophils enter bloodfrom bone marrow. Figure 21.4, step 1
Innatedefenses Internaldefenses Inflammatorychemicalsdiffusingfrom theinflamed siteact as chemotacticagents. Capillary wall Basementmembrane Endothelium 1 2 Leukocytosis.Neutrophils enter bloodfrom bone marrow. Margination.Neutrophils clingto capillary wall. Figure 21.4, step 2
Innatedefenses Internaldefenses Inflammatorychemicalsdiffusingfrom theinflamed siteact as chemotacticagents. Capillary wall Basementmembrane Endothelium 1 2 3 Leukocytosis.Neutrophils enter bloodfrom bone marrow. Margination.Neutrophils clingto capillary wall. Diapedesis.Neutrophils flatten andsqueeze out of capillaries. Figure 21.4, step 3
Innatedefenses Internaldefenses Inflammatorychemicalsdiffusingfrom theinflamed siteact as chemotacticagents. 4 Chemotaxis.Neutrophilsfollow chemicaltrail. Capillary wall Basementmembrane Endothelium 1 2 3 Leukocytosis.Neutrophils enter bloodfrom bone marrow. Margination.Neutrophils clingto capillary wall. Diapedesis.Neutrophils flatten andsqueeze out of capillaries. Figure 21.4, step 4
Antimicrobial Proteins • Interferons (IFNs) and complement proteins • Attack microorganisms directly • Hinder microorganisms’ ability to reproduce
Interferons • Viral-infected cells are activated to secrete IFNs • IFNs enter neighboring cells • Neighboring cells produce antiviral proteins that block viral reproduction
Innate defenses Internal defenses Virus 1 Virusenters cell. New viruses Viral nucleic acid 5 Antiviralproteins blockviralreproduction. 2 Interferongenes switch on. DNA Nucleus mRNA 4 Interferonbindingstimulates cell toturn on genes forantiviral proteins. 3 Cell producesinterferonmolecules. Interferon Host cell 2Binds interferon from cell 1; interferon induces synthesis ofprotective proteins Host cell 1Infected by virus;makes interferon;is killed by virus Figure 21.5
Innate defenses Internal defenses Virus 1 Virusenters cell. Viral nucleic acid Nucleus Host cell 2Binds interferon from cell 1; interferon induces synthesis ofprotective proteins Host cell 1Infected by virus;makes interferon;is killed by virus Figure 21.5, step 1
Innate defenses Internal defenses Virus 1 Virusenters cell. Viral nucleic acid 2 Interferongenes switch on. DNA Nucleus Host cell 2Binds interferon from cell 1; interferon induces synthesis ofprotective proteins Host cell 1Infected by virus;makes interferon;is killed by virus Figure 21.5, step 2
Innate defenses Internal defenses Virus 1 Virusenters cell. Viral nucleic acid 2 Interferongenes switch on. DNA Nucleus mRNA 3 Cell producesinterferonmolecules. Interferon Host cell 2Binds interferon from cell 1; interferon induces synthesis ofprotective proteins Host cell 1Infected by virus;makes interferon;is killed by virus Figure 21.5, step 3
Innate defenses Internal defenses Virus 1 Virusenters cell. Viral nucleic acid 2 Interferongenes switch on. DNA Nucleus mRNA 4 Interferonbindingstimulates cell toturn on genes forantiviral proteins. 3 Cell producesinterferonmolecules. Interferon Host cell 2Binds interferon from cell 1; interferon induces synthesis ofprotective proteins Host cell 1Infected by virus;makes interferon;is killed by virus Figure 21.5, step 4
Innate defenses Internal defenses Virus 1 Virusenters cell. New viruses Viral nucleic acid 5 Antiviralproteins blockviralreproduction. 2 Interferongenes switch on. DNA Nucleus mRNA 4 Interferonbindingstimulates cell toturn on genes forantiviral proteins. 3 Cell producesinterferonmolecules. Interferon Host cell 2Binds interferon from cell 1; interferon induces synthesis ofprotective proteins Host cell 1Infected by virus;makes interferon;is killed by virus Figure 21.5, step 5
Interferons • Produced by a variety of body cells • Lymphocytes produce gamma (), or immune, interferon – stimulates macrophages to killer status • Most other WBCs produce alpha () interferon – reduce inflammation • Fibroblasts produce beta () interferon – reduce inflammation • Interferons also activate macrophages and mobilize NKs
Interferons • Functions • Anti-viral – in the cell being defended the cell produces PKR ( Protein Kinase RNA) – this blocks the virus from making new proteins in the host cell – blocks at the ribosome • Reduce inflammation • Activate macrophages and mobilize NK cells • Genetically engineered IFNs for • Antiviral agents against hepatitis and genital warts virus – alpha and Beta Interferons • Multiple sclerosis treatment – Beta Interferon
Complement • ~20 blood proteins that circulate in an inactive form • Include C1–C9, factors B, D, and P, and regulatory proteins • Major mechanism for destroying foreign substances