Emergency Delivery
Emergency Delivery. Presence Regional EMS November 2013 CE. Objectives. Describe the normal changes that occur in a woman’s body during pregnancy Outline the steps of assessment of the pregnant patient Differentiate between the 3 stages of labor Describe the indications of imminent delivery.

Emergency Delivery
E N D
Presentation Transcript
Emergency Delivery Presence Regional EMS November 2013 CE
Objectives • Describe the normal changes that occur in a woman’s body during pregnancy • Outline the steps of assessment of the pregnant patient • Differentiate between the 3 stages of labor • Describe the indications of imminent delivery
Objectives (cont.) • Explain the steps of a normal delivery • Outline the steps for care of the newborn • Recognize complicated deliveries including malpresentation, maternal hemorrhage, meconium staining and multiple gestations.
Introduction • Most infants are delivered in a hospital. • Occasionally, the birth process moves faster than the mother expects. • You must then decide whether to: • Stay on the scene and deliver the infant • Transport the patient to the hospital
Normal Changes in Pregnancy • Many normal changes occur in the body that are not all directly related to the reproductive system. • Respiratory changes • Cardiovascular changes • Musculoskeletal changes
Normal Changes in Pregnancy • Rapid uterine growth occurs in the second trimester. • As the uterus grows, it pushes up on the diaphragm and displaces it. • Respiratory capacity changes, due to brocho-dilation with increased respiratory rates and decreasing minute volumes.
Normal Changes in Pregnancy • Blood volume gradually increases to: • Meet the increased needs of the fetus • Allow for adequate perfusion of the uterus • Prepare for the blood loss during childbirth • Number of red blood cells will increase • The patient is able to clot faster. • The patient’s heart rate increases up to 20%.
Vasodilation • To accommodate the increased blood volume the pregnant woman’s blood vessels dilate • Keeps blood pressure lower • Gives the “rosy glow” of pregnancy
Vital Signs • Do not mistake normal vital signs of pregnancy for signs of shock. • Normal pulse: 10–15 beats faster • Blood pressure: 10–15 mmHg lower • 30–35% blood loss before significant blood pressure change
Patient Assessment • Childbirth is seldom an unexpected event, but there are occasions when it becomes an emergency. • Dispatch protocols usually include the dispatcher asking simple questions to determine whether birth is imminent.
Patient Assessment • Scene Size-Up • Your safety is a priority. • Take standard precautions. • Gloves and eye protection are a minimum if delivery is already begun or is complete. • If time allows, a mask and gown should also be used. • Consider calling for additional resources. • Form a general impression. • The general impression should tell you whether the patient is in active labor or if you have time to assess and address other possible life threats
Patient Assessment • Evaluate • Level of consciousness • Airway • Breathing • Circulation • Transport decision • If delivery is imminent, prepare to deliver at the scene. • If delivery is not imminent, prepare the patient for transport.
History Taking • Obtain a thorough obstetric history: • Her expected due date • Any complications that she is aware of • If she has been receiving prenatal care • Her thorough medical history
Physical Exam • Assess the major body systems. • Assess for fetal movement. • For a pregnant patient in labor, focus on contractions and possible delivery. • If you suspect that delivery is imminent, check for crowning.
Vital Signs • Include pulse; respirations; skin color, temperature, and condition; and BP • Pay attention to tachycardia and hypotension or hypertension. • Hypertension, even mildly elevated BP, may indicate more serious problems.
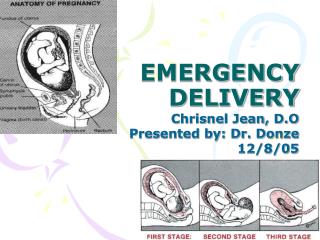
Stages of Labor • First Stage – dilation • Begins with first uterine contraction and ends when the cervix is completely dilated. • “Bloody” show. • Rupture of amniotic sac. • Contractions increase in frequency and intensity. • May last longer for woman having first child.
Stages of Labor • Second Stage – Expulsion • Begins with complete cervical dilation and ends with delivery of the baby. • Contractions are close together and last longer. • Mother has urge to “push.” • Perineum may tear. • Crowning.
Stages of Labor • Third stage – placental • Begins once the baby is delivered and ends when the placenta is expelled. • Placenta typically delivered 5 to 20 minutes after the baby. • Gush of blood. • Uterus becomes smaller. • Umbilical cord lengthens. • Maternal urge to push.
Preparing for Delivery • Consider delivering the infant at the scene when: • Delivery can be expected within a few minutes • A natural disaster, inclement weather, or other environmental factor makes it impossible to reach the hospital
Preparing for Delivery • To determine if delivery is imminent, ask the patient: • How long have you been pregnant? • When are you due? • Is this your first baby? • Are you having contractions? • How far apart? • How long do they last?
Preparing for Delivery • To determine if delivery is imminent, ask the patient (cont.): • Do you feel as though you will have a bowel movement? • Have you had spotting or bleeding? • Has your water broken? • Were any of your previous children delivered by cesarean section?
Preparing for Delivery • Delivery can probably be expected within a few minutes, if the following signs and symptoms are present: • Crowning has occurred. • Contractions are 2 minutes apart or closer, and they are intense and last from 60 to 90 seconds. • The patient feels the infant’s head moving down the birth canal (sensation of the urge to defecate). • The patient has a strong urge to push. • The patient’s abdomen is very hard.
Preparing for Delivery • To help determine potential complications, ask: • Have you had problems in a previous pregnancy? • Do you use drugs, drink alcohol, or take any medications? • Is there a chance of multiple birth? • Does your doctor expect complications?
Preparing for Delivery • If the patient has delivered before, she may be able to tell you whether she is about to deliver. • If she has an extremely firm abdomen or feels the need to push, the infant’s head is probably pressing on the rectum. • Visually inspect the vagina to check for crowning.
Preparing for Delivery • Use proper BSI. • Act calm and reassuring. • Prepare OB kit. • Push away or remove mother’s clothing while preserving modesty. • Place the mother in a semi-Fowler’s position. • Pad under and around the mother’s hips (raise hips approximately 4” with padding)
Delivering the Baby • Support the head as it emerges, using caution not to push on soft area of scalp. • Once the head emerges, determine if the umbilical cord is around the infant’s neck (nuchal cord). • If it is, use two fingers to slip the cord over the infant’s shoulder. If you cannot move the cord, place two clamps 2 to 3 inches apart and cut between the clamps. Remove the cord from around the neck. • Suction airway with bulb suction, always suction mouth first then nose.
Delivering the Baby • Support the head and upper body as the shoulders deliver. • Handle the infant firmly but gently as the body is delivered. • Suction airway again.
WARNING • Guide the baby in the delivery • Never pull!!!
Post Delivery Care • Dry off the infant and wrap in a blanket or towel. • Place the infant on one side, with the head slightly lower than the rest of the body. • Wrap the infant so only the face is exposed. • Keep the blanket or towel warm.
Post Delivery Care • Clamp and cut the umbilical cord • Place clamps 2-3 inches apart, first one approximately 7 inches from baby. • Wait until pulsation stops, then cut with sterile scissors. • Monitor end for bleeding, if bleeding occurs place another clamp proximal to the initial clamp.
Post Delivery Care • Delivery of the placenta • Placenta is attached to the end of the umbilical cord. • It should deliver within 30 minutes. • Never pull on the umbilical cord. • Once it delivers, wrap the placenta and take to the hospital so it can be examined. • If the mother continues to bleed, transport promptly to the hospital, and massage the uterus to stimulate contractions.
Post Delivery Care • Record the time of birth in your patient care report. • The following are emergency situations: • More than 30 minutes elapse, and the placenta has not delivered • There is more than 500 mL of bleeding before delivery of the placenta. • There is significant bleeding after the delivery of the placenta.
Neonatal Evaluation and Resuscitation • Perform APGAR Score at 1 minute and 5 minutes after birth • Newborns should begin breathing spontaneously within 15-30 seconds after birth • Heart rate should be ≥ 120 beats / minute
Neonatal Evaluation and Resuscitation • Many infants require some form of stimulation, including: • Positioning the airway, drying, warming, suctioning, or tactile stimulation • Use the inverted pyramid concept
Neonatal Evaluation and Resuscitation • To maximize the effects of these measures, follow these tips: • Position the infant on the back with the head down and the neck slightly extended. • Suction the mouth and then the nose. • In addition to drying the head, back, and body with dry towels, rub the back and flick or slap the soles of the feet.
Neonatal Evaluation and Resuscitation • Evaluate skin color: • If skin is pink or pink with peripheral cyanosis, monitor. • If skin is cyanotic throughout, administer supplemental OXYGEN by blow-by technique.
Neonatal Evaluation and Resuscitation • Evaluate respirations • If respirations are adequate but cyanosis is present, administer supplemental oxygen by blow by technique. • If neonate is apneic or respirations are inadequate, ventilate with BVM and 100% oxygen at 40-60 breaths/minute. • Reassess every 30 seconds.
Neonatal Evaluation and Resuscitation • Evaluate the heart rate at the base of the umbilical cord or the brachial artery. • If the heart rate is > 100, initiate transport keeping infant warm and re-assess frequently • If the heart rate is 60-100, begin assisted respirations with a bag mask device and 100% oxygen • Reassess every 30 seconds until heart rate and respirations are normal