Download
1 / 71
740 likes | 2.09k Vues
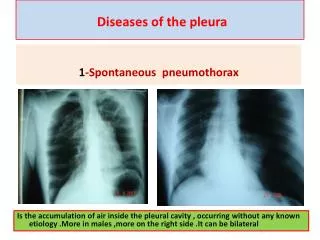
Diseases of Pleura. ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara , Nepal. Negative intrapleural pressure: ~ 5mm. PLEURISY . Disease process involving the pleura and giving rise to pleuritic pain evidence of pleural friction Common feature of

E N D
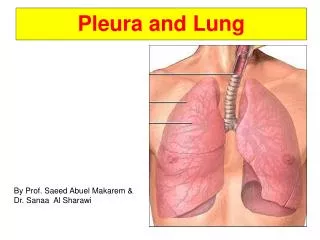
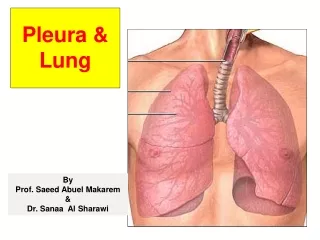
Diseases of Pleura ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal
PLEURISY • Disease process involving the pleura and giving rise to • pleuritic pain • evidence of pleural friction Common feature of • Pulmonary infection • Infarction • Malignancy • Primary pleural involvement – in T.B.
Clinical features • Characteristic symptom – Pleural pain On examination: • Rib movement restricted – reduced chest expansion • Pleural rub may be present • may only be heard in • deep inspiration • near pericardium - pleuro-pericardial rub
Loss of the pleural rub and diminution in the chest pain indicate • Either recovery or • development of a pleural effusion • Normal X-ray does not exclude pulmonary cause for pleurisy • pulmonary infection which may not have been severe enough • may have resolved before the chest X-ray was taken
The accumulation within the pleural space of • Serous fluid - • Frank pus - • Blood - pleural effusion empyema haemothorax
Pleural fluid accumulates increased hydrostatic & decreased osmotic pressure – ‘Transudate’ • Increased microvascular pressure • due to disease of pleural surface or injury in the adjacent lung ‘Exudate’
Transudate • Congestive heart failure • Cirrhosis (hepatic hydrothorax) • Hypoalbuminemia • Nephrotic syndrome • Myxedema • Constrictive pericarditis
Tuberculous Parapneumonic causes Malignancy (carcinoma, lymphoma,mesothelioma) Pulmonary embolism Pancreatitis Collagen-vascular conditions (rheumatoid arthritis, SLE) Asbestos exposure Trauma Postcardiac injury(Dressler’s)syndrome Esophageal perforation Radiation pleuritis Drug use Chylothorax Meigs syndrome Sarcoidosis Yellow nail syndrome Exudate
Clinical assessment • Symptoms and signs of pleurisy often precede the development of an effusion in patients with • Tuberculosis • underlying pneumonia • pulmonary infarction • connective tissue disease
Particular attention should be paid to a recent history of • contact with tuberculosis • respiratory infection • presence of heart disease • liver or renal disease • occupation (e.g. exposure to asbestos) • risk factors for thromboembolism
BREATHLESSNESS - only symptom related to effusion and its severity depends on the size rate of accumulation
Manifest when pleural effusions >300 mL On inspection: • Fullness of chest on affected side • Reduced expansion of chest • Tracheal shift with Trail’s sign - observed with effusions of > 1000 mL • Prominence of lower part of sternocleidomastoid due to tracheal deviation
On palapation • Trachea & apex beat shifted to opposite side • Decreased tactile fremitus
Displacement toward the side of the effusion is an important clue to obstruction of a lobar bronchus
Percussion: • Dullness on percussion- stony dull • obliteration of tympanitic percussion note over Traube’s space in left sided effusion • Level of dullness goes up in axilla • Dullness over grocco’s triangle
surface markings • left sixth rib • left midaxillary line • left costal margin Traube's space
Upper margin of fluid Grocco’s triangle XII th rib
Grocco's Paravertebral Triangle • Triangular area of dullness at the back of chest on the healthy side • Base – horizontally along the XII th rib • Apex – at the level of upper margin of fluid on diseased side • Internally – vertebral line • Externally – line joining the apex and lateral base
Ascultation • Decreased or absent breath sounds • Pleural friction rub may be present ONLY WHEN EFFUSION IS SMALL
zone of compensatory emphysema compressed lung Findings at the upper level of moderate effusion
Increased VF, egophony & bronchial breath sounds Skodaic resonance – percussion Dull on percussion Absent Br sound Egophony: high-pitched nasal or bleating quality sound
Possible findings at the upper level of dullness in case of moderate pleural effusion: 1. lung is compressed • Increased vocal fremitus & aegophony – nasal quality of sounds transmitted • Bronchial breath sound 2. there may be a zone of compensatory emphysema above it • Skodaic resonance on percussion
1.Chest X ray • P A view: minimum of 200cc of fluid required to produce blunting of costophregnic angles in • Lateral view: 60 ml • lateral decubitus Xray: 10 ml
200 ml fluid required to produce this shadow 60 ml in lateral view 10 ml in decubitus Xray
X ray tube X rays
Some atypical pleural effusions • Localised effusions: previous scarring or adhesions in the pleural space • Subpulmonary effusion: Pleural fluid localised below the lower lobe simulates an elevated hemidiaphragm • Fluid localised within an oblique fissure may produce a rounded opacity simulating a tumour
Phantom tumor -Pleural effusion in Interlobar fissure
2. USG of thorax: • Can detect even less than 10 ml • Can differentiate between pleural thickening & effusion • USG guided needle aspiration in small effusion
1.Biochemical analysis • Protein • L.D.H. 3. Sugar – low in bacterial infections & Rh. arthritis 4. A.D.A – high (>42) in T.B. & some fungal infections 5. Amylase – high in pancreatitis, oesophageal rupture, malignancy Required for calculating LIGHT’S CRITERIA
6.pH Low pH suggests infection rheumatoid arthritis ruptured oesophagus advanced malignancy
2. Microscopic examination Predominant cell type provides useful information and cytological examination is essential Polymorphs suggest bacterial infection Lymphocytes: tuberculous High ADA + Pl. fluid lymphocyte/neutrophil > 0.75 – Highly diagnostic of tuberculous pleural effusion Malignant cells ma be seen in malignancy
3.Gram stain may suggest parapneumonic effusion 4.ELISA or PCR Helpful in diagnosing T.B. if acid-fast bacilli are not seen 5. Cultures: positive in 30 to 70% (Enzyme-linked immunosorbent assay) (Polymerase chain reaction)
4. Pleural biopsy May be required if all fails • With all methods combined yield is close to 95%
Combining pleural aspiration with biopsy increases the diagnostic yield • Ultrasound or CT guided biopsy with Abrams needle is most frequently employed
Pleural aspiration and biopsy • Abrams needle