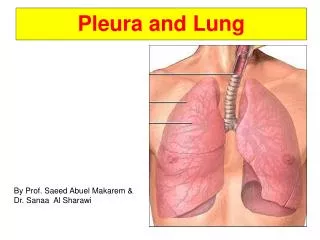
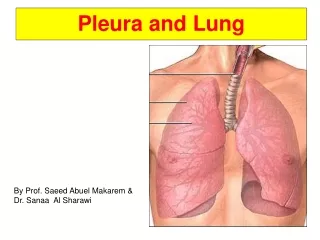
Pleura t ypes
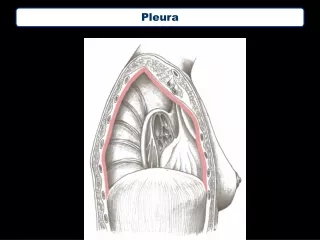
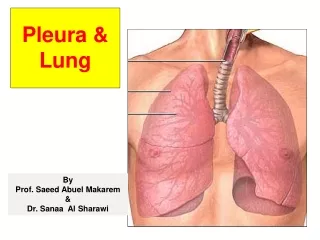
Pleura t ypes. There are two types of pleura : * visceral pleura * parietal pleura The parietal pleura is subdivided into * mediastinal pleura * costal pleura * diaphragmatic pleura * cervical pleura. margins of parietal pleura and pleural recesses.


Pleura t ypes
E N D
Presentation Transcript
Pleura types • There are two types of pleura :* visceral pleura* parietalpleura • The parietal pleura is subdivided into * mediastinal pleura* costal pleura* diaphragmatic pleura* cervical pleura
margins of parietal pleura and pleural recesses • Margins of the parietal pleura :* Anterior margin* Inferior margin • pleural recesses* Costomediastinal recess* Costodiaphragmatic recess
Nerve supply of pleura The parietal pleura somatic nerves The costal and peripheral parts of diaphragmatic pleurae intercostal nerves The mediastinal and central part of diaphragmatic pleurae phrenic nerves The visceral pleurae No sensory innervation autonomic nerves derived from the anterior and posterior pulmonary plexuses
Blood supply and lymphatics of pleura Blood supply intercostal- internal thoracic and musculophrenic vessels the vessels of the thoracic wall The parietal pleura The visceral pleurae Bronchial vessels
lymphatics *Lymphatices of the parietal pleura join those in the thoracic wall draining into intercostal-posterior mediastinal- *parasternal-diaphragmatic Lymph nodes *Lymphatices of the visceral pleurae join those of lung (bronchopulmonary Lymph nodes )
pulmonary tuberculosis disease (T.B) • Definition • Tuberculosis, commonly known as TB, is a bacterial infection that can spread through the lymph nodes and bloodstream to any organ in your body. It is most often found in the lungs. Most people who are exposed to TB never develop symptoms because the bacteria can live in an inactive form in the body. But if the immune system weakens, such as in people with HIV or elderly adults, TB bacteria can become active. In their active state, TB bacteria cause death of tissue in the organs they infect. Active TB disease can be fatal if left untreated.
Causes of TB disease • The bacterium that causes TB is called Mycobacterium .Only people who have active TB infections can spread the TB bacteria. Coughing, sneezing, even talking can release the bacteria into the surrounding air, and people breathing this air can then become infected. This is more likely to happen if you're living in close quarters with someone who has TB or if a room isn't well ventilated . People who are at greater risk for TB infection include the elderly, homeless people and people with weakened immune systems from HIV or AIDS. Once a person is infected, the bacteria will settle in the air sacs and passages of the lungs and, in most cases, will be contained by the immune
Symptoms of TB disease • Symptoms develop gradually, and it may take many weeks before you notice that something's wrong and see your doctor. Although the TB bacteria can infect any organ (e.g., kidney, lymph nodes, bones, joints) in the body, the disease commonly occurs in the lungs. • Common symptoms include: • 1-coughing that lasts longer • than 2 weeks with green, yellow, • or bloody sputum • 2-weight loss • 3-fatigue • 3-fever • 5-night sweats • 6-chills • 7-chest pain • 8-shortness of breath • 9-loss of appetite
How to diagnose TB ? Step one
Step two Step three
Step four Step five
Medications for treatment TB : Other considerations :
Pulmonary cavity filled with variable things *The lungs are lined on the outside with two thin layers of tissue called pleura. The space between these two layers is called the pleural space. Normally, there is only a small amount of lubricating fluid in this space. *Liquid and/or air accumulates in this space between the lungs and the ribs from many conditions : _The liquid is called a pleural effusion_the air is called a pneumothorax.
Most pleural effusions are complications emanating from metastatic malignancy (movement of cancer cells from one part of the body to another). • Most malignant pleural effusions are detected and controlled by thoracentesis. • Thoracentesis is also performed as a diagnostic measure. • In these cases, only small amounts of material need to be withdrawn.
Symptoms • Symptoms of a pleural effusion include :1- breathing difficulty 2- chest pain 3- fever 4- weight loss 5- cough 6- edema.
Complications • Removal of air is often an emergency procedure to prevent suffocation from pressure on the lungs. • Negative air pressure within the chest cavity allows normal respiration. • The accumulation of air or fluid within the pleural space can eliminate these normal conditions and disrupt breathing and the movement of air within the chest cavity
Treatment • Fluid removal is performed to reduce the pressure in the pleural space and to analyze the liquid. • thoracentesis was traditionally used to remove blood from the chest cavity. This is rare now that the placement of a thoracostomy tube has proven to be a more effective and safer method.
ThoracentesisAreas of • The usual place to tap the chest is below the armpit (axilla). Under sterile conditions and local anesthesia, a needle, a through-the-needle-catheter, or an over-the-needle catheter may be used to perform the procedure. Overall, the catheter techniques may be safer. Fluid or air is withdrawn. Fluid is sent to the laboratory for analysis. If the air or fluid continue to accumulate, a tube is left in place and attached to a one-way system so that it can drain without sucking air into the chest.
Precautions • Care must be taken not to puncture the lung when inserting the needle. Thoracentesis should never be performed by inserting the needle through an area with an infection. An alternative site needs to be found in these cases. Patients who are on anticoagulant drugs should be carefully considered for the procedure.
Treatment of hemothorax • A hemothorax is managed by removing the source of bleeding and by draining the blood already in the thoracic cavity. Blood in the cavity can be removed by inserting a drain (chest tube) in a procedure called a tube thoracostomy. Usually the lung will expand and the bleeding will stop after a chest tube is inserted
Treatment of hydrothorax • Acute thoracentesis is seldom required for treatment of an acute and severe presentation of a hydrothorax with respiratory compromise. The simple drainage of the peritoneal cavity and avoidance of overnight dwells in the supine position can correct the problem in some patients. The persistence of hydrothorax requires permanent obliteration of the pleuro-peritoneal communication with pleurodesis using autologous blood, talc, tetracycline, surgical or thoracoscopic correction or video-assisted thoracoscopic (VATS) talc pleurodesis
Treatment for pneumothorax • The treatment pathway will depend on the severity of the pneumothorax. If you have had a small pneumothorax, you may not require any treatment but you will still be advised to have a chest X-ray to check that the pneumothorax has cleared and you may also be given painkillers. • If you have had a larger pneumothorax doctors may need to release some of the trapped air. This is usually done by inserting a very fine tube into the pleural space, with a syringe fitted to the end of the tube, which sucks in the trapped air. If the pneumothorax is larger, a bigger tube may be needed to remove more air and sometimes the tube is left in place for a few days to allow the tear in the lung tissue to heal. Local anaesthetic will be given prior to the tube being inserted into the chest wall to prevent pain. • If you have had a pneumothorax, you have a higher risk of developing another pneumothorax in the future. If you suffer recurrent pneumothorax you may be advised to have surgery
Treatment of pyothorax • The recommended treatment for most cases of pyothorax isclosed-tube thoracostomy, together with chest drainage, lavage and instigation of appropriate antimicrobial drug treatment based on culture and sensitivity Use of fine needle