Download

1 / 86
990 likes | 1.98k Vues
SPINAL CORD TRAUMA. KATHY GARVIN, RN, BA, MICN Department of Emergency Medicine LAC+USC Medical Center Level I Trauma Center. OBJECTIVES. Identify significant mechanisms of injury that put patient at high risk for spinal cord injury

E N D
SPINAL CORD TRAUMA KATHY GARVIN, RN, BA, MICN Department of Emergency Medicine LAC+USC Medical Center Level I Trauma Center
OBJECTIVES • Identify significant mechanisms of injury that put patient at high risk for spinal cord injury • Identify the signs and symptoms of a spinal cord injury and the basic pathophysiology behind the findings • Identify Nursing assessments and interventions • Identify Goals of Intervention
Paramedic Notes • Jon Wilhite and 3 friends, in a small car, are hit by a drunk driver. • 0010: Fullerton emergency officials get report of a high-speed collision • 0017: 1st fire engine on scene. Passenger in the right rear seat, does not have a pulse • 0019: 1st ambulance arrives. Fire crew prepares to cut away roof to get to female driver, Jon, seated behind her, and a badly injured passenger, in the front. The driver dies moments later. • Jon is unconscious and appears to have only minor cuts. Paramedics follow protocol. C-collar, back board and lift him out of car. • 0034: Ambulance speeds to medical center at UC Irvine. Paramedic notes unequal pupils.
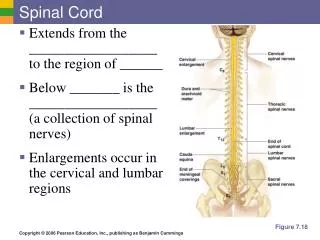
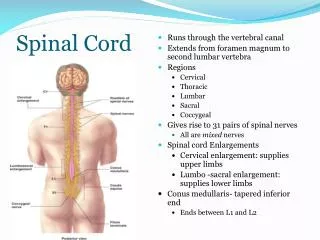
Vertebral Column 7 cervical - vulnerable 12 Thoracic – attached to ribs 5 Lumbar – junction with thoracic vulnerable Fused Sacrum and Coccyx
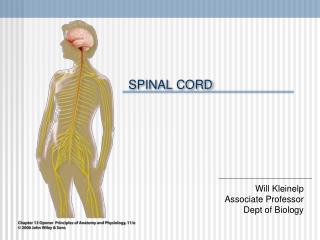
Spinal Cord Anatomy • 31 pairs of nerves exit the cord • Carry both motor and sensory • Ligaments provide support • Discs act as shock absorbers • Spinal arteries provide blood • Cord is mass of nerve tissue • Extends from foramen magnum • to L-2
SPINAL CORD INJURY (SCI) • An insult to the spinal cord resulting in changed neurological function • Motor • Sensory • Autonomic • May be temporary or permanent • Injuries tend to be physically, emotionally and financially devastating
CLASSIFICATION • Tetraplegia: (quadriplegia) • Cervical region injury • Loss of muscle strength to all four extremities • Most critical: support respiratory function • Paraplegia • Injury to the spinal cord in the • Thoracic • Lumbar • Sacral segments • T12 and L1 are the most common level
EPIDEMIOLOGY • World Wide: young men • Mechanism depends on area of world • Falls • Motor vehicle crash • Work/Construction • Spine weakened by disease
MECHANISM OF INJURY • In the United States: • Automobile accidents • High speed • Ejection. rollover • Falls • Greater than 4.5 meters/15 feet (or 3x height) • Slip and fall: rare except in elderly • Diving into shallow pool • Violence • Blunt • Penetrating • Sports
SITE OF INJURY AND NEUROLOGIC LEVEL C5 Most common site of injury T12 / L1 most common injuries
PRIMARY AND SECONDARYSPINAL CORD INJURY • Primary Spinal Cord Injury • Initial physical damage to spinal cord or its structures • Physical cord damage due to mechanical insult • Neurons passing through injury site are physically disrupted and exhibit diminished myelin thickness
PRIMARY AND SECONDARY INJURY • Secondary Spinal Cord injury: • Progressive pathological responses to initial injuries • Hemorrhage into cord compartments • Inflammatory response to initial insult (Biochemical cascade, progressive edema and cell necrosis) • Hypoxia due to local and systemic hypoperfusion • Systemic hypotension from other injuries (bleeding) or neurogenic shock • Collectively damage intact neighboring tissue • Symptoms: paralysis and loss of sensation to areas innervated below the general level of the injury
NEUROGENIC VS SPINAL SHOCK • Spinal Shock • Short term loss of spinal cord function • Injury at any cord level • Starts 30-60 minutes following a spinal cord injury • Results in flaccid paralysis, areflexia and anesthesia below the level of injury • Resolves in days to weeks
NEUROGENIC VS. SPINAL SHOCK • Neurogenic Shock • A form of distributive shock • Injury at T6 and above • Impairment of Sympathetic Pathway • Loss of vasomotor tone causing hypotension and venous pooling • Loss of sympathetic innervation to heart: bradycardia • Loss of thermoregulation: poikilothermia • Loss of ability to sweat: anhydrosis
CORD SYNDROMES • Complete cord syndrome: Complete loss of motor and sensory function below the level of the traumatic lesion. • Incomplete cord syndromes: • Variable neurologic findings • Partial loss of sensory and/or motor function below the level of injury • Central Cord syndrome • Anterior Cord syndrome • Posterior Cord Syndrome • Brown-Sequard syndrome
COMPLETE CORD SYNDROME • Associated with blunt or penetrating trauma results in complete disruption of spinal cord • Characterized by • complete loss of motor and sensory function • Below the level of the traumatic lesion • Symptoms that remain >24 hours generally are permanent.
COMPLETE CORD SYNDROME Dermatomes correspond clinically to each nerve root. Sensation is described and impairment defined by the dermatomes affected
ANTERIOR CORD SYNDROME Commonly a flexion injury – burst fracture, herniated disc • Involves a lesion causing variable loss of • Motor function • Pain • Temperature sensation • Preservation of • Proprioception • Vibration • Touch
CENTRAL CORD SYNDROME • Most common incomplete syndrome • Hyperextension injury, often seen in the elderly • Usually involves a cervical lesion • Motor weakness • Upper extremities > lower extremities • Sensory loss is variable • Sacral sensory sparing • More likely to lose pain and/or temperature sensation than proprioception and/or vibration. • Sensation of burning in the hands or arms common
POSTERIOR CORD SYNDROME • condition caused by lesion of the posterior portion of the spinal cord • Can be caused by an interruption to the Posterior spinal artery • Very rare condition • Loss of proprioception, vibration and touch • Preservation of motor pain and temperature
BROWN-SÉQUARD SYNDROME • Associated with a hemisection lesion of the cord from penetrating trauma • Involves ipsilateral loss of proprioception and motor function • Contralateral loss of pain and temperature sensation
BIOMECHANICS • Hyperextension • Rear-end crashes • Damage to anterior ligaments and bony dislocations • Hyperflexion • Head-on crashes • Wedge fractures, Facet dislocations, teardrop fractures • Rotational • “Spinning crashes • Rupture of the posterior ligament and or anterior fracture/dislocation of vertebral body • Axial loading • Diving accidents • Deformity of vertebral column
Vertebral Column Injuries • Ligaments – critical for cord stability • Vertebral Fractures: Stable vs. Unstable • Stable only if no potential for progressive impingement or injury to the spinal cord at any time • Unstable until proven otherwise Vascular Structures: critical for cord viability Discs: may herniate and compress cord or nerve roots
Odontoid Fracture • unstable injury • most common in kids up to 8 years old (75%) • adults: 10 % of cases
VENTILATION AND SPINAL CORD INJURY • Injury of C3 And above • Loss of phrenic nerve • Likely to cause death from respiratory arrest • Injury between C3 and C5 • Loss of diaphragmatic innervation • Likely to cause respiratory insufficiency • Injury between C6 and T8 • Involves loss of intercostal and abdominal muscle function • Causing increase work of breathing
SCIWORA Spinal Cord Injury without Radiologic Abnormality • Seen most often in children • Associated with • Transient ligamentous deformation with spontaneous reduction • Occult disc herniation • Cord hemorrhage • Fibrocartilaginous emboli • Traumatic aortic dissection • Devastating if missed
SPINAL CORD INJURY UNTIL PROVEN OTHERWISE IF: • Significant mechanism of injury • high speed motor vehicle collision • Fall from a height • Diving accident • Electrocution • Direct neck trauma • Head or Neck pain associated with trauma • Motor or sensory deficits • Altered Level of Consciousness • Distracting Injury
NURSING ROLE • Early identification of potential Spinal Cord Injury • Recognize significant mechanism of injury • Identify signs and symptoms • Good Assessment Skills • Interventions that protect patient from secondary harm
Primary and Secondary Surveys • Primary Survey – Assess for life threatening injuries, if identified, stop immediately and address before moving on • Airway with Spinal Cord Precautions • Breathing and Ventilation • Circulation • Disability – mental status • Exposure
Primary and Secondary Surveys • Secondary Survey • Complete head to toe and focused assessment • History • Everything else
Hospital Notes • 0042: Ambulance arrives to hospital’s ER. Paramedic gives report and trauma team takes over. “They all had a job. They were all doing it at once.” • 0044: 2nd ambulance leaves the crash scene with 2nd patient on the backboard. • 0050: Ultrasound (FAST) and X-ray no bleeding in lungs or abdomen • Blood pressure stable. • Hypothermic • 0101: CT – atlanto-occipital dislocation (internal decapitation), broken ribs, shoulder blade and collapsed lungs. Fracture at the base of the skull, bleeding into his brain.
AIRWAY AND SPINAL PROTECTION • Airway with simultaneous spinal protection • Manually hold head/neck in line • Inspect the airway using jaw thrust (if able) • Tongue, secretions, blood, vomit, edema, foreign body, retropharyngeal hematoma • Gentle, frequent suction (avoid vagal stimulation and hypoxia) • Quick check of head and neck for life threatening injury/bleeding
AIRWAY WITH SPINAL STABILIZATION • Oxygen • Oral-tracheal intubation with in-line stabilization is the preferred method • Any episode of hypoxia can lead to cord ischemia and further injury • Plan for: rigid C-collar (if able), head supports, long board, log roll patient • Minimal movement/manipulation of spine!