SPOT QUESTIONS 3
SPOT QUESTIONS 3. Q1 50 yr old man with this pre-op CT ABDO and intra-op finding. 1. Diagnosis 2. Aetiology 3. Surgical management at operation. Q2 50 yr female with dysphagia 1. Diagnosis 2. Pathophysiology 3. Presentation 4. Other investigations 5. Management. Q3 70 yr male

SPOT QUESTIONS 3
E N D
Presentation Transcript
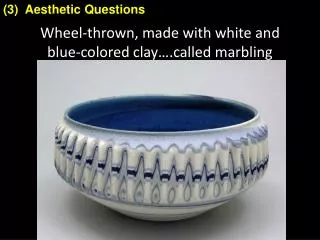
Q1 50 yr old man with this pre-op CT ABDO and intra-op finding. 1. Diagnosis 2. Aetiology 3. Surgical management at operation
Q2 50 yr female with dysphagia 1. Diagnosis 2. Pathophysiology 3. Presentation 4. Other investigations 5. Management
Q3 70 yr male 1. Diagnosis 2. Presentation 3. Pathophysiology 4. Investigations 5. Management
Q4 Small bowel at colonoscopy 1. Diagnosis 2. Macroscopic features 3. Microscopic features
Q5 1. What is this procedure and findings? 2. What risks do you advise about this procedure? 3. What can be done to minimise the risks?
Q6 1. Describe what you see 2. Pathophysiology of this sign 3. Operation recommended
Q1 50 yr old man with this pre-op CT ABDO and intra-op finding. 1. Diagnosis 2. Aetiology 3. Surgical management at operation
SB intussusception • Aetiology: • Invagination (or 'telescoping') of one loop of intestine (intussusceptum) into another (intussuscipiens) • Idiopathic or lead point (tumour, infective, congenital). Rare in adults & usually SB tumour (benign or malignant). • More often in children (age 3mths – 2yrs) with syndrome of colicky pain, vomiting, passage of blood per rectum, and palpable sausage-shaped mass. Due to enlarged Peyer's patch from viral infection, with peak incidence in spring and mid winter. In infants only 5% have recognisable lesion eg polyp, Meckel's diverticulum, duplication or tumour. • Complete resection adhering to basic oncological principles – clear margins, draining lymph nodes (although may have haematogenous spread), leaving a well vascularised tension-free secure anastomosis.
50 yr female with dysphagia 1. Diagnosis 2. Pathophysiology 3. Presentation 4. Other investigations 5. Management
Achalasia (“failure to relax”). Differentials: benign strictures due to GORD, GO junction or oesophageal carcinoma (pseudoachalasia) [consider in any patient >60yrs age, recent onset dysphagia (<6mths), excessive weight loss].[Described in 1672, treated with whale bone bougie, term coined in 1929] • Partial or complete loss of ganglia cells in the myenteric plexus (Auerbach’s) combined with an inflammatory infiltrate. Get LES which fails to relax appropriately and loss of peristalsis in distal 2/3rds oesophagus. Unknown aetiology, but 2 theories exist: (1) a degenerative disease of neurons; (2) infections of the neurons by a virus (eg herpes zoster) or another infectious agent (eg Chagas' disease – American trypanosomiasis trypanosoma cruzii) , where get destruction of parasymp ganglion cells in GI, cardiac, urinary and respiratory tracts).
With degeneration of myenteric plexus of Auerbach, lose postganglionic inhibitory fibres (containing NO and VIP), which mediates LES relaxation. Sparing of postganglionic cholinergic stimulation, hence unopposed cholinergic stimulation, which increases LES resting pressure and decreases LES relaxation. In response to swallowing there is no propagation of peristaltic waves, but rather simultaneouscontractions. • Oesoph manometry findings: • Elevated LOS pressure • Incomplete or absence of LOS relaxation on swallowing • Absence of peristalsis in oesophagus • Elevated intra-oesophageal pressure
Presentation • History: • Incidence 1/100 000, M:F 1:1, age typically 25-60 yrs, caucasians > others, average symptom duration at diagnosis: 2-5 years • solid dysphagia 90-100% (75% also to liquids) • post-prandial regurgitation 60-90% (fermented debris) • chest pain (usually at time of meal) 33-50% • Heartburn (from stasis and fermentation undigested food) 25-45% • weight loss • nocturnal cough and recurrent aspiration • Examination: • Usually non-contributory, but NB: dentition, aspiration signs, nutritional status, cancer nodal METS
Investigation: • Plain CXR film (air-fluid level, wide mediastinum, absent gastric bubble, pulmonary infiltrates) • Barium oesophagram (dilated esophagus with taper at LES - “birds beak” appearance) • good screening test (95% accurate) • Oesophageal manometry (absent peristalsis, ↓ LES relaxation, & resting LES >45 mmHg) *gold standard* • Endoscopy to rule out tumour of GO junction. Findings: atonic oesophagus, dilated, tortuous, LES closed tightly and does not open with air insufflation, mucosal changes due to chronic irritation with food stagnation (erythema, friable mucosa, ulceration, Candidal infection)
Management: • No cure, treatment aimed at relief of symptoms. Options include medical, endoscopic and surgical interventions. Surgery is most effective option. • Medical: nitrates and calcium channel blockers • 50-70% initial response; <50% at 1 year • limitations: tachyphylaxis and side-effects • Endoscopic: • Botulinum toxin (prevents ACH release at NM junction restoring balance btwn excitatory and inhibitory neurotransmitters) • 90% initial response; 60% recurrence at 6 months • Inflammatory reaction makes subseq myotomy difficult
Endoscopic: pneumatic dilation (disrupt circular muscle) • 60-95% initial success; 60% at 5 years • recent series suggest 20-40% will require re-dilation • risk of perforation 1-13% (usually 3-5%) [immediate L thoracotomy, closure of perforation, myotomy]; death 0.2-0.4%; post-dilatation GOR 25-35%. • Surgical: Laparoscopic Heller's cardiomyotomy and partial fundoplication, open or minimally-invasive approaches, oesophagectomy if failed myotomy & dilatation • >90% initial response; 85% at 10 years; 70% at 20 years (85% at 5 years with min. inv. techniques) • <1% mortality; <10% major morbidity • 10-25% acutely develop reflux, up to 52% develop late reflux. Barrett’s in 13%, 35-fold increased risk oesophageal Ca (espec men). Recommend OGD every 3-4 yrs post-op.
Management: • Results of medical, interventional, and surgical procedures all point to surgery as being the safest and most effective treatment. • Balloon dilation vs Botox injections symptom remission at 1 year 89 vs 38% • Balloon dilation vs surgery perforation rates 4% vs 1% mortality rate 0.5 vs 0.2% result 'excellent' 60 vs 85% • Laparosocpic versus open myotomy laparoscopic have shorter hospital stay, less pain, less 'heartburn'
70 yr male 1. Diagnosis 2. Presentation 3. Pathophysiology 4. Investigations 5. Management
Pharyngoesophageal diverticulum (Zenker's diverticulum). Differentials to consider include: oesophageal stricture, achalasia, oesophageal cancer. • M:F 1.5:1, most >60 yrs age. Present with dysphagia,regurgitation of undigested food (aspiration and pneumonia possible), halitosis, gurgling sounds in the neck. 30% have associated GORD. • Progressive herniation of mucosa & submucosa originates in posterior wall of oesophagus in triangular area of weakness (Killian triangle), limited inferiorly by cricopharyngeus muscle and superiorly by the inferior constrictor muscles. Due to either lack of coordination btwn pharyngeal contraction and opening time of the UES, or to hypertensive UES. (UES is at level of cricoid cartilage approx 15cm from incisors on OGD). As diverticulum enlarges, it tends to deviate from midline, mostly to the left.
Barium swallow shows position and size of diverticulum, or a prominent cricopharyngeal bar without diverticulum. Hiatal hernia present in some patients. CXR Oesophageal manometry shows lack of coordination btwn pharynx and cricopharyngeus muscle and often a hypertensive UES. May also show hypotensive LES and abnormal oesophageal peristalsis. Ambulatory pH monitoring determines GORD. Endoscopy (flexible) may be dangerous and cause perforation. Consider rigid endoscopy if performed. • Operative excision of diverticulum and myotomy of cricopharyngeus muscle & upper 3cm of posterior oesophageal wall via left neck approach. For small diverticula (<2cm) myotomy alone is sufficient. Transoral endoscopic approach with stapling device to ablate the septum btwn diverticulum and cervical oesophagus, is another option for diverticula 3-6cm in size. If GORD is present, correct this prior to dividing UES to avoid aspiration.
Small bowel at colonoscopy 1. Diagnosis 2. Macroscopic features 3. Microscopic features
SB Crohn's (ileal) • Macroscopic: • Any part of the GI tract • Apthous ulcerations, serpiginous ulcerations • Skip lesions eg strictures separated by normal intestine • Thickened mucosa, fissuring of mucosa, submucosa oedema, pseudopolyps → giving “cobblestone” appearance • Serosal inflammation and adhesions • Fistulation and abscesses • Thickened mesentery with “fat creeping”
Microscopic • Oedema in lamina propria and submucosa • Intact glands (cf gland destruction, loss of goblet cells & crypt abscess in UC) • May be foci of pyloric metaplasia. Lymphoid hyperplasia in lamina propria and submucosa. Hyperplasia of muscularis mucosae. Lymphatic dilatation. Fibrosis. Increase in number of smooth muscle fibres in submucosa. • Transmural chronic inflammatory infiltrate (lymphocytes, plasma cells, eosinophils, histiocytes - some containing prominent lysosomal inclusions, mast cells) • Non-caseating granulomas (50-70%) • Full thickness penetration of ulcers and fissures resulting in abscesses and fistulas • Focal inflammation walls of veins and arteries • Skip lesions
1. What is this procedure and findings? 2. What risks do you advise about this procedure? 3. What can be done to minimise the risks?
Endoscopic retrograde cholangiopancreatography (ERCP) with distal CBD stones and dilated extra- and intra-hepatic biliary tree. Pancreatic duct evident. ? Previous cholecystectomy. • Complications (total major complication rate 10%): • Procedure-related mortality 0.5% (age-independent) • Acute pancreatitis (6-8%) [diagnostic 3%, therapeutic 5%] • Cholangitis • Perforation – pharynx, oesophagus, duodenal • Haemorrhage • Incomplete duct clearance • Need for further procedures or surgery • Sphincterotomy with risk of long-term stricturing • Aspiration • Reaction to sedative & analgesic medications
Minimising risks: • Identify those at risk for ERCP-induced pancreatitis • Female sex, Sphincter of Oddi dysfunction, Normal serum bilirubin levels, History of recurrent pancreatitis • Identify and address procedure-related risk factors: • Pancreatic duct contrast injection, Balloon dilation of the sphincter, Operator inexperience, Use of needle-knife & site of sphincterotomy • If incomplete duct clearance, leave biliary stent in-situ • Give prophylactic antibiotics (eg Ciprofloxacin 200mg IV 2hrs pre-procedure) • Give post-procedural diclofenac 100mg supp. to reduce incidence pancreatitis
1. Describe what you see 2. Pathophysiology of this sign 3. Operation recommended
Positive Pemberton sign. Mild facial plethora at rest and an enlarged heterogeneous thyroid gland with probably impalpable lower poles. When the patient raises both arms above his/her head, get marked facial congestion, cyanosis, and venous engorgement of the scalp. • Pemberton sign occurs when the thoracic inlet becomes obstructed during positional changes, resulting from compression of the major veins. Cannot accommodate increase venous return from elevated limbs. It is a common manifestation of retrosternal goiter but may also occur with lung carcinoma, lymphoma, thymoma, or thoracic aortic aneurysms. • Total thyroidectomy. Or treatment of the underlying cause: CTx (+/- RTx) for lymphoma, CTx/RTx for lung carcinoma, endovascular or open repair thoracic aortic aneurysm.
Q7 Angiogram 1. Describe what you see and what other features to look for 2. Likely presentation 3. Management
Q8 1. Describe what you see 2. Investigations 3. Management
Q9 24 year male 1. Likely diagnosis 2. Possible causes 3. Investigations 4. Management
Q10 26yr male MVA. [Compound wound actually in proximal 1/3rd lower leg] 1. Describe what you see 2. Investigations 3. Management
Q11 Colonoscopy finding: 1. What is likely diagnosis and chromosomal abnormality? 2. Other problems in this condition? 3. What operation? 4. What follow-up?
Q12 Fluid in LUQ after subtotal gastrectomy 1. Differential diagnosis? 2. Management
Q13 Lymphoedema right leg, patient in their 40's, and present for 5 years 1. Likely diagnosis 2. Investigations 3. Treatment
Angiogram 1. Describe what you see and what other features to look for on this imaging 2. Likely presentation 3. Management
SMA angiogram with occlusion approx 7cm from its origin. In absence of stigmata for vascular disease or collaterals, most likely cause is thromboembolus from fibrillating heart or mural thrombosis post MI. Imaging note – absent intestinal gas, distension of SB and colon up to splenic flexure, blunt plicae, thickened bowel wall, intra-mural or portal venous gas (late signs).Aetiology: arterial emboli 50% (mural thrombus infarcted LV or clot in fibrillating LA with mitral stenosis), thrombosis 25%, [dissecting or fusiform aortic aneurysm (rare), non-occlusive 20%]. Occlusion smaller mesenteric arteries in connective tissue or other systemic disorders, or cocaine ingestion. • Sudden onset severe central or diffuse ABDO pain disproportionate to objective clinical abdominal signs. Usually elderly patient with associated cardiac or peripheral vascular disease or risk factors. May have history of chronic intestinal ischaemia. Vomiting and diarrhoea (bloody a late sign), and ABDO distension may be present. Peritoneal irritation indicates full-thickness bowel infarction and irreversibility of process. SMA thrombosis has more insidious onset of symptoms.
Management • General • Venous access (often CVL), NGT, IDC inserted • Fluid and electrolyte resuscitation • IV broad spectrum antibiotics • Organ supports and correction of metabolic acidosis • Liaise & discuss with patient and relatives, anaesthetists, intensivists, interventional radiologists • No diagnostic lab test. May have leukocytosis, raised amylase (50%), raised CK-BB, base deficit. Imaging – as previous. Short of mesenteric arteriography or CT angiogram, imaging studies cannot be relied on to definitively rule out acute mesenteric ischaemia. Barium studies show “thumbprinting” and disordered motility (either slow or rapid).
Management • Specific • In angio suite with SMA clot and no signs of irreversible ischaemia (eg peritonism, mural or portal venous gas) → lysis of clot via angiography with catheter placed immediately proximal to clot (streptokinase, rtPA, APSAC). • Most need laparotomy. Options: open/close for large length intestinal infarction; embolectomy for embolic disease with heparinisation or vascular surgeon aortomesenteric bypass grafting for thrombosis with pre- & post-op intra-arterial infusion papaverine (30-60mg/hr); resect infarcted bowel and either exteriorise both bowel ends or leave stapled off ends in-situ, laparostomise and return for re-exploration at 24-48hrs; Post-op ICU with cardiac and respiratory and often renal supports, inotropes and antibiotics, heparinize, re-look laparotomy as necessary. Cardiac ECHO for cause. [Prognosis – up to 90% mortality with mesenteric infarction, better outcome with embolic cause]
Q8 Advanced breast cancer 1. Describe what you see 2. Investigations 3. Management
Locally advanced right breast cancer (T4 - ? inflammatory) with right upper limb lymphoedema. Likely T4b or T4d and N2 disease clinically. • Triple assessment – clinical examination, MAMMO/USS, core biopsy with immuno-histochemical analysis for hormonal sensitivities (ER/PR/Her-2); CT scan of CHEST/ABDO; bone scan; routine bloods – FBC, RENL, LFTs, calcium, phosphate • Above investigations followed by discussion in BREAST MDT meeting and URGENT referral to Oncology. Likely up front chemo-radiotherapy aiming for loco-regional disease and symptom control. Endocrine therapies per sensitivities. Palliative mastectomy and axillary dissection according to response to above therapies as discussed in MDT forum. Prognosis is very poor. Breast care nurse specialist and cancer support group input. Palliative care service referral.
Q9 24 year male 1. Likely diagnosis 2. Possible causes 3. Investigations 4. Management
Gynaecomastia (probably physiological) with enlargement of ductal and stromal tissue. (Incidence: 1/3rd adult males, ½ pubescent boys) • Causes of gynaecomastia in males: • PHYSIOLOGICAL (High serum oestradiol to testosterone ratio) • neonate, puberty, elderly • IDIOPATHIC (most) • PATHOLOGICAL:
Causes of gynaecomastia in males: • PATHOLOGICAL • Drug-induced (eg hormonal supplements (oestrogens), alcohol, cimetidine, digoxin, phenothiazines, methyldopa, TCAs, some antihypertensives, spironolactone, cyproterone acetate) • Increased oestrogen production (eg hepatoma, testicular, pituitary and adrenal tumours or paraneoplastic syndrome – bronchial carcinoma) • Decreased oestrogen clearance (eg cirrhosis, haemochromatosis, Wilson’s disease) • Decreased testosterone production (eg Klinefelter's syndrome, mumps orchitis, bilateral cryptorchidism, acquired testicular failure eg irradiation, hypopituitarism) • Testicular feminisation syndrome
Management • Adolescents do not require investigation. Reassure that is a benign and self-limiting condition. 75% better in 2y • Rest guided by history & examination findings: • TFTs, LFTs, aFP, bHCG, prolactin • Scrotal USS or liver imaging (CT SCAN) • FNA/core biopsy for discrete breast lesion • Treatment of any underlying cause. • Subcutaneous mastectomy for debilitating symptoms only.
Q10 26yr male MVA. [Compound wound actually in proximal 1/3rd lower leg] 1. Describe what you see 2. Investigations 3. Management
Compound # right proximal tibia/fibula with apparent neurovascular compromise to distal limb (compressed vs severed deep popliteal artery and nerves from displaced tibial plateau #) • EMST primary survey and adjuncts with realignment and xray lower limb # (if position not held with splint, maintain manually). Clinical examination +/- Doppler assessment of distal vessels. Primary survey x-rays – C-spine, CXR, Pelvic. • Aim of management is to identify and treat immediate life & limb threatening injuries. Resuscitation and direct pressure to open wound after realignment with in-line traction for # immobilization. Tetanus prophylaxis, antibiotics for compound wound, analgesia. Prompt operative management (Orthopaedic, Vascular +/- Plastics) to salvage limb and restore distal vascular supply as matter of priority. Consider intra-operative angiography to confirm vascular patency/exclude intimal tear. May require fasciotomy to treat or prevent compartment syndrome. Early amputation may give best functional outcome in some scenarios. Document findings and treatments accurately.
Q11 Colonoscopy finding: 1. What is likely diagnosis and chromosomal abnormality? 2. Other problems in this condition? 3. What operation? 4. What follow-up?
Familial Adenomatous Polyposis (FAP) from mutant APC gene (a tumour suppressor and gate-keeper gene) on long arm of Chr5 (5q21). Autosomal dominant. No FHx in 30%. Responsible for 0.5% all CRC. Causes florid adenomatous polyposis commencing in teens/early 20's and progressing to adenoCa in ~100%, often before age 30yrs. • Extra-colonic manifestations: • Osteomas (espec skull + mandible) and sebaceous cysts = Gardner’s Syndrome • Gastroduodenal polyps - gastric hamartomas, duodenal adenomas (~100%, 5% become malignant) • Intra-ABDO desmoid tumours (10%) Desmoid = tendon-like, fibrous. Dermoid = resembling skin • Pigmented ocular lesions & brain tumours = Turcot syndrome. Congenital hypertrophy retinal pigment epi. (CHRPE) (80%) • Also increased risk of periampullary, thyroid and CNS tumours, carcinoid of ileum, hepatoblastoma.
Surgical options: • Panproctocolectomy and end ileostomy (best option oncologically) (rarely performed these days, unless rectal cancer already present) • Restorative panproctocolectomy (IPAA) (higher operative morbidity, usually better functional outcome) • Subtotal colectomy & ileorectal anastomosis. (NB will require surveillance of rectal stump). Risk rectal Ca 15% at 15yrs hence convert to ileal pouch-anal anastomosis after age 40yrs. Preserves pelvic nerve innervation until child-bearing complete. • 2 groups present for prophylactic surgery: screen-detected members of known FAP family (usually in teenage years) and symptomatic individuals (mostly in their 30's). Colectomy before age 20 is desirable to prevent CRC (5% risk by age 20).