Open Fracture Management
Open Fracture Management. P. Blachut Division of Ortho Trauma Vancouver General Hospital University of British Columbia. Introduction Assessment Classification Management. Open fractures. Goals of Fracture Management. Fracture healing with satisfactory length and alignment


Open Fracture Management
E N D
Presentation Transcript
Open Fracture Management P. Blachut Division of Ortho Trauma Vancouver General Hospital University of British Columbia
Introduction • Assessment • Classification • Management Open fractures
Goals of Fracture Management • Fracture healing with satisfactory length and alignment • Avoidance of complications • infection • nonunion • malunion • stiffness • Early restoration of function
Fracture Healing • Biologic factors • Biomechanical factor
Avoidance of Complications (Infection) • No necrotic tissue • No dead space • No contamination • Well vascularized tissue
Early Restoration of Function • Early mobilization • Stable fixation • Early wound healing • Avoid excessive scarring • Early wound coverage with quality tissue • Preservation of “critical tissues” • Nerves • Tendons
Therefore: • The soft tissues are paramount to the successful management of fractures
A bone healing complication with good soft tissues is easier to deal with than a complication with poor soft tissues
Consequences of an Associated Soft Tissue Injury • healing potential • resistance to infection • contamination
Assessment • Look for associated life threatening injuries!!! • Carefully assess and document neurovascular status
ATLS (Advanced Trauma Life Support) • Primary Survey • A irway • B reathing • C irculation • D isability • E xposure • Secondary Survey
Compartment Syndrome • Always look for in fractures with soft tissue injuries • Open fractures - up to 10% have compartment syndrome
Amputation vs. Salvage • Multidisciplinary decision • Based on the assessment of likely ultimate function of limb compared to function with amputation
Factors Favoring Amputation • Warm ischemia time > 8 hrs • Severe crush • minimal remaining functional tissue • Chronic debilitating disease • Severe polytrauma • Mass casualty • complexity of reconstruction
Classification - Open Fractures • Reflection of amount of energy imparted and consequently, the prognosis • Skin wound size • Level of contamination • Extent of soft tissue injury/ periosteal stripping • Fracture configuration
Classification - Open Fractures • Classification can really only be done at the completion of debridement
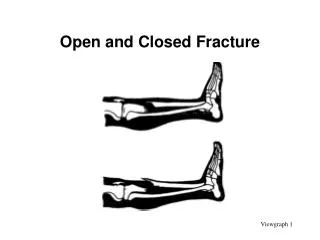
Classification - Open Fractures • Open injuries • Gustilo & Anderson • AO
Open Fracture - Gustilo Classification • Type I • Small wound • Inside out • No/minimal contamination • Minimal soft tissue trauma • Low energy fracture pattern
Open Fracture - Gustilo Classification • Type II • Moderate wound • Some contamination • Some muscle damage • Moderate energy fracture pattern
Open Fracture - Gustilo Classification • Type III • Large wound • Significant comtamination • Major soft tissue trauma • crushing • periosteal stripping • High energy fracture pattern
Open Fracture - Gustilo Classification • IIIA • enough soft tissue to cover bone • IIIB • insufficient soft tissue • need flap (local, free) • IIIC • vascular injury requiring repair
Open Fracture - Gustilo Classification • Type III - Additional Factors • Barnyard • Shotgun • High velocity gunshot • Displaced segmental fracture • Neglected open fracture (> 8 hrs) • Bone loss
Management • First aid • Emergency Room • Definitive • Rehabilitation
First Aid • Control bleeding • direct pressure • Realign • further soft tissue damage/ compromise • Splint • comfort • further damage
Emergency • First aid if not already given • Remove gross debris/irrigate/dress/ splint • Tetanus prophylaxis - if necessary • Antibiotics
Emergency • The open wound should be assessed and documented only once
Antibiotics • ? Prophylactic vs. treatment Closed with operative Rx Cephalosporin Grade I Grade II / III Add aminoglycoside High Risk Add penicillin
Antibiotics • Antibiotics can not compensate for an inadequate surgical management
Timing of Administration of Antibiotics • The Prevention of Infection in Open Fractures An Experimental Study of the Effect of Antibiotic Therapy Worlock, et al JBJS 1988 No antibiotics 1-4 hrs post-inoculation 1 hr. pre-inoculation 91% infection 51% infection 30% infection
Antibiotics • The Role of Antibiotics in the Management of Open Fractures • Patzakis, et al JBJS, 1974 Control Pen./Streptomycin Cephalothin 13.9% infection 9.7% infection 2.3% infection
Definitive Treatment • Wound excision • Wound extension • Debridement • Irrigation • Bone stabilization • Wound dressing • +/- re-debridement • Early wound closure/coverage
Timing of Operative Intervention • General standard - within 6-8 hours • Not evidence based!!
Operating Room • Scrub/remove gross debris/ irrigate • Double setup • debridement/irrigation • bone stabilization if internal fixation planned • Tourniquet • apply/not inflated • in case of bleeding
Wound Excision • Excise crushed/ contaminated skin edge
Wound Extension • Sufficient extension to fully evaluate and treat soft tissue injury (approximately 1 diameter of limb) • Anticipate incisions for bony stablization/soft tissue reconstruction • Avoid incision that will compromise skin further
Debridement • Layer by layer • Remove all devitalized and contaminated tissue (including bone)
Debridement - Objective: • To leave a wound with: • No/minimal contamination • Well vascularized tissue for healing and to resist infection
Debridement • “When in doubt, take it out”
Irrigation • 10 litres for significant wounds • saline • ? antibiotics • ? pulsed lavage • ? detergent
Irrigation • Improves visualization • Float out necrotic tissue • Flush out debris • Reduce bacterial population
Irrigation • The solution to pollution is dilution
Stabilization The Prevention of Infection in Open Fractures: An Experimental Study of the Effect of Fracture Stability Worlock, et al Injury 1994
Bony Stabilization • Second prep if internal fixation • Principles • Minimize further trauma • Sufficient stability to allow early rehab • Should not impede subsequent soft tissue management • Restoration of anatomy
Bony Stabilization • Diaphyseal Fractures • Humerus • Forearm • Femur • Tibia ORIF IM nail
Bony Stabilization • Articular Fractures • primary ORIF • spanning external fixator + / - articular ORIF delayed ORIF • external fixation