DISORDER OF SKIN APPENDAGES
610 likes | 1.27k Vues
DISORDER OF SKIN APPENDAGES. TOPICS INCLUDED. Acne vulgaris Rosacea Miliaria Excessive hair loss Excessive hair growth. DISORDER OF SENACEOUS GLANDS Acne vulgaris. Sebaceous glands. Develop embryologically from hair germs, but a few free glands arise from the epidermis.

DISORDER OF SKIN APPENDAGES
E N D
Presentation Transcript
TOPICS INCLUDED • Acne vulgaris • Rosacea • Miliaria • Excessive hair loss • Excessive hair growth
DISORDER OF SENACEOUS GLANDS Acne vulgaris
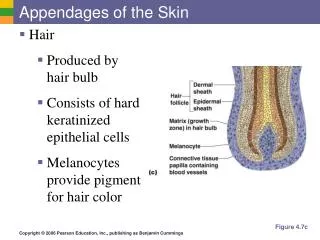
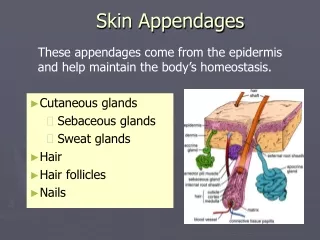
Sebaceous glands Develop embryologically from hair germs, but a few free glands arise from the epidermis. The glands themselves are multilobed Contain cells full of lipid(sebum), which are secreted (holocrine secretion-when whole cell is secreted into the lumen)
Sebum is discharged into the upper part of the hair follicle. It lubricates and waterproofs the skin, and protects it from drying; It is also mildly bactericidal and fungistatic.
ACTIVITY Androgenic hormones, especially dihydrotestosterone, stimulate sebaceous gland activity. Human sebaceous glands contain 5α-reductase, 3α- and 17α- hydroxysteroid dehydrogenase Convert weaker androgens to dihydrotestosterone, which in turn binds to specific receptors in sebaceous glands, increasing sebum secretion. So , not the levels of circulating androgens but an enhanced target organ sensitivity which is important.
Acne Acne is a disorder of the pilosebaceous apparatus predominantly affecting the peripubertal popln andcharacterized by comedones, papules, pustules, cysts and scars.
Prevalence Nearly all teenagers have some acne (acne vulgaris). It affects the sexes equally, starting usually between the ages of 12 and 14 years, tending to be earlier in females. The peak age for severity in females is 16–17 and in males 17–19 years. Variants of acne are much less common.
Causes of Acne vulgaris Many factors combine to cause acne characterized by chronic inflammation around pilosebaceous follicles
Sebum Sebum excretion is elevated.
Hormonal changes • Androgens (from the testes, ovaries,adrenals and sebaceous glands themselves) are the main stimulants of sebum excretion, • In most of the cases the level of the androgens are within normal limit but there is enhanced end organ sensitivity (incred.activity of enzyme 5-alpha reductase) • Other hormones (e.g. thyroid hormones and growth hormone) have minor effects too.
Poral occlusion Occluded by keratinous plug induced by: • Both genetic and environmental factors (e.g. some cosmetics) • Reduced levels of linoleic acid in sebaceous gland secetions of acne patient • Results in vicious cycle of retentin of sebum to growth of microbs. Distention of follicle eventually ruptures releasing pro-inflammatory chemicals into dermis stimulating intense inflammation.Theductal epithelium also produces cytokines and an inflammatory cascade is triggered.
Bacterial Propionibacterium acnes Acts as a source of antigenic stimulation,triggering a type IV inflammatory response. Produce extracellular enzymes which attract inflammatoy cells.
Factors modifying Acne Genetic predisposition(mode of inheritence not clear) The condition is familial mostly with severe cystic acne Identical twins Cosmetics Menstrual cycle Psychological factors- anger, anxiety
Presentation Polymorphic eruption: papules,pustule,comedones,nodules and cysts Lesion heals with depressed or hypertrophic scarring and Post-inflammatory hyperpigmentation can follow.
Lesions are confined to the face, shoulders, upper chest and back. Open comedones (blackheads), because of the plugging by keratin and sebum of the pilosebaceous orifice on the skin surface, or Closed comedones (whiteheads), caused by plugging below the skin surface. Associations : Most have a background of greasy skin(seborrhea) with patulous follicular openings(pores)
Acne associated with virilization May be caused by an androgen-secreting tumour of the adrenals, ovaries or testes or, rarely, congenital adrenal hyperplasia Acne accompanying the polycystic ovarian syndrome is caused by modestly raised circulating androgen levels
Variants of acne • Infantile acne may follow transplacental stimulation of a child’s sebaceous glands by maternal androgens. • May present at birth or may last for upto 3yrs • Its morphology is like that of common acne and it may be the forerunner of severe acne in adolescence.
Papulopustular lesions in an odd distribution. The patient played the violin (‘fiddler’s neck’) Mechanical. Excessive scrubbing, picking, or the rubbing of chin can rupture occluded follicles.
Drug-induced Steroid-induced acne in a seriously ill patient. • Lesions are monomorphic and esp. over back ,face may be involved • Suspicion should be raised when acne, dominated by papulopustules rather than comedones appear suddenly in a nonteenager • And coincides with the prescription of a drug known to cause acneiform lesions • Corticosteroids • Androgenic • Anabolic steroids • Gonadotrophins • Oral contraceptives • Lithium, iodides, bromides, antituberculosis and anticonvulsant therapy can all cause an acneiform rash.
Acne due to cosmetics Cosmetics esp. oil based or other topical preparations may induce comedone formation or precipitate inflammation around hair follicles.
Conglobates (gathered into balls) is the name given to a severe form of acne with all of the above features as well as abscesses or cysts with intercommunicating sinuses that contain thick serosanguinous fluid or pus. On resolution, it leaves deeply pitted or hypertrophic scars, sometimes joined by keloidal bridges. Hyperpigmentation is usually transient, it can persist, particularly in those with an already dark skin.
Fulminans Acne fulminans It is a rare variant in which conglobate acne with ulcerated and crusted lesion and is accompanied by Fever, arthralgia,myalsia and a high erythrocyte sedimentation rate (ESR).
chloracne Exogenous Tars, chlorinated hydrocarbons, oils and oily cosmetics can cause or exacerbate acne. Suspicion should be raised if the distribution is odd(forearm, legs)or unusal age(mid age male) or if comedones predominate
Excoriated This is most common in young girls. Obsessional picking otherwise mild acne Results in excoriations on face while primary lesions not visible
Late onset This too occurs mainly in women Is limited to the chin. Nodular and cystic lesions are predominant. It is stubborn and persistent.
Tropical This occurs mainly on the trunk and may be conglobate.
Acne after facial massage • Acne following (3-6 wks later) in abt 30% of patients • Nodules with few comedones • Along mandibular region
Course Acne vulgaris clears by the age of 23–25 years in 90% of patients, Some (5% of women and 1% of men) still need treatment in their thirties or even forties.
Investigations None are usually necessary. Cultures are occasionally needed to exclude a pyogenic infection, an anaerobic infection or Gram-negative folliculitis.
Any acne, including infantile acne, that is associated with virilization needs investigation to • Exclude an androgen-secreting tumour of the adrenals, ovaries or testes • To rule out congenital adrenal hyperplasia
Differential diagnosis Rosacea affects older individuals Pyogenic folliculitis Hidradenitis suppurativa is associated with acne conglobata, but attacks the axillae and groin. Pseudofolliculitis barbae, caused by ingrowing hairs, occurs on the necks of men with curly facial hair and clears up if shaving is stopped.
Treatment General measures Acne frequently has marked psychological effects. Even those with mild acne need sympathy, optimistic approach is essential, and regular encouragement is worthwhile. Local hygiene, diet, stress
Local treatment • 1 Regular gentle cleansing with mild soap and water • Benzoyl peroxide. • This antibacterial agent plus decreases inflammation • applied only at night initially, but can be used twice daily if this does not cause too much dryness and irritation. • Retinoic Acid(RA)/tretinoin • The vitamin A (retinol) analogues (tretinoin, isotretinoin, adapalene,(recently introducedand less irritent) ,tazarotene)normalize follicular keratinization, and reduce sebum production and reduce inflammation,decrease p.acne • They are especially effective against comedones. • Patients should be warned about skin irritation (start with small amounts) and photosensitivity.
The weakest preparation should be used first, and applied overnight on alternate nights. Sometimes, after a week or two, it will have to be stopped temporarily because of irritation. The combination of benzoyl peroxide in the morning and tretinoin at night has many advocates. Isotretinoin 0.05%, 0.025%, 0.1% Other agents Azelaic acid :reduce post acne hyperpigmentation Alpha hydroxy acids eg. Glycolic acid
Topical antibiotics Topical clindamycin, erythromycin and sulfacetamide Cosmetic camouflage- Cover-ups help some patients, especially females, whose scarring is unsightly. They also obscure post-inflammatory pigmentation.
Systemic treatment Antibiotics • tetracycline includes:doxycycline and minocycline mostly used and less frequently erythromycin and azithromycin • Used in mod. to severe acne and in those who are having psy. problem • Tetracycline-1gm,doxycycline-100mg,minocycline-100mg, erythromycin-1gm, azithromycin-250mg daily for long periods of time up to 6 mths or even longer. • It should be taken on an empty stomach, 1 h before meals or 4 h after food
Oral antibiotics should be combined with topical agents because then it is possible to withdraw the antibiotic and maintain in topical therapy. • Side effects: • GI disturbance • Vaginal candidiasis • Resistance • Grayish pigmentation in case of minocycline • To be avoided in pregnancy.
Hormonal • Antiandrogenics only for females • Cyproterone acetate, a combined antiandrogen–oestrogen treatment • Combined oral contraceptives • Spironolactone • Isotretinoin- for severe intractable acne • Severe acne,conglobata • Relapses • Side effects:dryness of skin, eye,nosebleed,initial aggravation of inflammation , myalsia, altered night vision and hair loss, avoided in pregnancy, • Careful monitoring with blood pictures and pregnancy test before and after starting rx
Acne scar treatment • Dermabrasion This helps to smooth out facial scars. • Lasers Skin resurfacing with CO2 and erbium lasers is rapidly replacing dermabrasion and chemical peeling • Dermal fillers Bovine collagen or hyaluronic acid fillers can be injected into depressed scars to improve their appearance. • Cryotherapy • Intralesionalcorticosterois
definition Rosacea is a chronic skin disorder characterized by erythema and telangiectasia and punctuated by acute episodic eruption of papules, pustules and swelling.
Rosacea affects the face of adults, usually women. • Although its peak incidence is in the thirties and forties, it can also be seen in the young or old. • It may coexist with acne.
cause • Rosacea is often seen in those who flush easily in response to warmth, spicy food, alcohol or embarrassment. • Hereditary component • Fair-skinned • Psychological abnormalities • chemicals, high dosages of isotretinoin, benzoyl peroxide and tretinoin. • A pathogenic role for the follicular mite dermodexfolliculorum as well as for microaerophilic gm negetive bacterium. Helicobacter pylori is suspected but has not been confirmed.
sites • The cheeks, nose, centre of forehead and chin are most commonly affected • The periorbital and perioral areas are usually spared • Lymphoedema, below the eyes and on the forehead, is seen in few cases • Intermittent flushing is followed by a fixed erythema and telangiectases. • Discrete domed inflamed papules, papulopustules and, rarely, plaques or nodules develop • No comedones or seborrhoea
Usually symmetrical Exacerbations and remissions
types 1. Papulopustular rosacea • Inflammatory lesions are predominant • Some permanent redness with red papules with some pus filled pustules (typically last 1-4 days); this subtype can be easily confused with acne.
Types.. 2. Erythematotelangiectatic rosacea • Vascular features predominate • Permanent redness / erythema with a tendency to flush and blush easily. • Small blood vessels are usually visible near the surface of the skin k/a telangiectases, sometimes associated with burning or itching sensations.
Types… 3. Phymatous type • This subtype is most commonly associated with rhinophyma, an enlargement of the nose. • Symptoms include thickening of skin, irregular surface, nodularities, and enlargement of nose. • Phymatousrosacea can also affect chin (gnatophyma), forehead (metophyma), eyelids (blepharophyma), and ears (otophyma). • Small blood vessels may be visible near the surface of the skin (telangiectases). .