Download
1 / 21
210 likes | 228 Vues
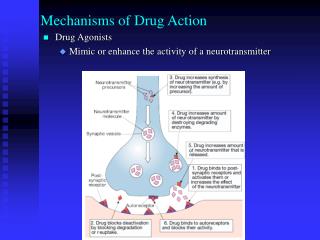
Antimicrobial treatments and their mechanisms of action. Regis P. Kowalski, MS,[M]ASCP Research Professor of Ophthalmology Executive Director of The Charles T Campbell Laboratory University of Pittsburgh, Pittsburgh, PA. The Charles T. Campbell Ophthalmic Microbiology Laboratory.

E N D
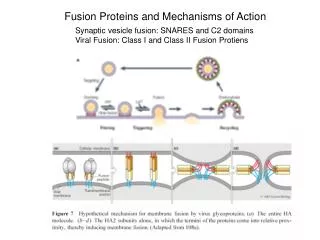
Antimicrobial treatments and their mechanisms of action Regis P. Kowalski, MS,[M]ASCP Research Professor of Ophthalmology Executive Director of The Charles T Campbell Laboratory University of Pittsburgh, Pittsburgh, PA The Charles T. Campbell Ophthalmic Microbiology Laboratory
Treatment Administration • Topical– Most common (conjunctivitis, keratitis, blepharitis, prophylaxis) • Intra-vitreal injection – endophthalmitis • Systemic – not commonly used • Subconjunctival – used to provide a constant flow of anti-infective to ocular surface.
Antibacterials • Antibiotics – No Topical Standards for Interpreting Susceptibility • Use Serum Systemic Susceptibility Standards - But we must assume that “The antibiotic concentrations reached in the ocular tissue by topical therapy is equal to or greater than the concentration of antibiotic in the blood serum”. • Ocular antibiotics are developed from systemic antibiotics for conjunctivitis, keratitis
Antibiotics Parameters Concentration–dependent fluoroquinolones, aminoglycosides Time-dependent vancomycin, cefazolin Bactericidal – kill FQs, vancomycin, Bacteristatic – inhibit erythromycin, azithromycin, sulfa Antiseptics – PI – kill immediately
Death and NO mutations MPC Death but possible mutations MBC No growth but viable MIC Growth Susceptibility Parameters
True Resistance Organism acquires resistance to an antibiotic. Resistance spreads to other patients No antibiotic to cover resistance
Class Mode of Action Primary Indication besides conjunctivitis Fluoroquinolones DNA synthesis keratitis, surgical prophylaxis (ciprofloxacin, ofloxacin, bactericidal Broad-spectrum coverage levofloxacin, gatifloxacin, moxifloxacin) besifloxacin Aminoglycosides protein synthesis keratitis, endophthalmitis (gentamicin, tobramycin, cell wall surgical prophylaxis amikacin) bactericidal Broad-spectrum coverage Cephalosporins cell wall keratitis, endophthalmitis (cefazolin, ceftazidime) bactericidal Gram-positive coverage Glycopeptides cell wall keratitis, endophthalmitis (vancomycin) bactericidal MRSA prophylaxis Gram-positive coverage Macrolides protein synthesis blepharitis (erythromycin, azithro) bacteristatic Gram-positive coverage Peptides cell wall blepharitis, keratitis (bacitracin, polymycin B) bactericidal Bac – GMpos PB – GMneg Sulfa drugs enzyme inhibitor keratitis, 2nd – line MRSA (sulfacetamide) bacteristatic Broad-spectrum coverage
Anti-Infective Test Batteries KeratitisEndophthalmitisConjunctivitis bacitracin vancomycin bacitracin vancomycin gentamicin erythromycin ciprofloxacin ciprofloxacin gentamicin ofloxacin ofloxacin ciprofloxacin polymyxin B cefazolin ofloxacin cefazolinamikacin trimethoprim tobramycinceftazidime polymyxin B sulfisoxazole cefoxitin tobramycin cefoxitin ampicillin sulfisoxazole gentamicin clindamycin azithromycin gatifloxacingatifloxacin gatifloxacin moxifloxacinmoxifloxacin moxifloxacin
Interactive Testing • “Synergism” is a positive effect where the combination of two antibiotics are more active than when either antibiotic is used independently. • An “additive effect” :The result with two drugs is equal to the sum of the results for each drug used separately.
Interactive Testing • “Antagonism” is a negative effect whereas the combination of both drugs is effectively less than the separate independent effects of both antibiotics. • An “indifferent interaction” indicates that both antibiotics react independent from each other.
Checkerboard Testing • Fractional Inhibitory Concentrations A/MICa + B/MICb = FIC index - “Synergism” = FIC index of 0.5 or less - “Additive” = >0.5 to 1.0 - “Indifferent” = 1.0to 2.0 - “Antagonism” = an FIC index greater than 2.0
Indifference GAT 0.06 B A K 1.0 0.06/0.06 + 1/1 = 2.0
Antagonism 1/0.25 + 256/256 = 5
Time-Kill Testing • A “Synergistic” interaction between two antibiotics is indicated with an additional 2 log decrease in colony counts with the antibiotic combination compared with the most effective single antibiotic. • An “antagonistic” interaction between two antibiotics is indicated with an additional 2 log increase in colony counts with the antibiotic combination compared to the most effective single antibiotic. • An “indifferent” effect between two antibiotics is indicated with an equivalent colony count between the antibiotic combination and the most effective single antibiotic.
A Synergism B A + B A Antagonism A + B B A Indifference A + B B
Keratitis Models New Zealand White Rabbits Two-eye design Corneas infected intrastromally with bacteria After 4 hours, treat with Anti-Infectives (5-8 hours) Determine viable bacteria Statistical Analysis Bactericidal Effect (3 log decrease)
In Vivo Interaction Testing Staphylococcus aureus Onset ≈ 99.9% kill 99.9 % Kill