Download
1 / 1
10 likes | 121 Vues
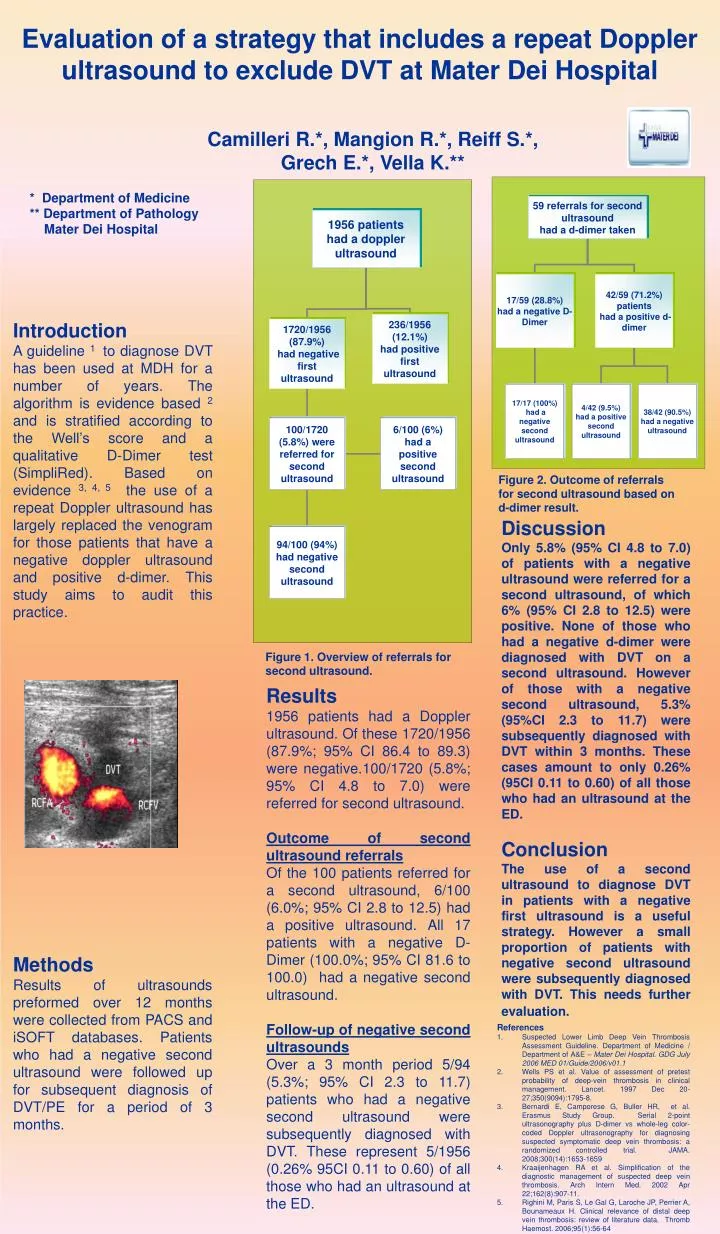
Evaluation of a strategy that includes a repeat Doppler ultrasound to exclude DVT at Mater Dei Hospital. Camilleri R.*, Mangion R.*, Reiff S.*, Grech E.*, Vella K.**. * Department of Medicine ** Department of Pathology Mater Dei Hospital. Introduction

E N D
Evaluation of a strategy that includes a repeat Doppler ultrasound to exclude DVT at Mater Dei Hospital Camilleri R.*, Mangion R.*, Reiff S.*, Grech E.*, Vella K.** * Department of Medicine ** Department of Pathology Mater Dei Hospital Introduction A guideline 1 to diagnose DVT has been used at MDH for a number of years. The algorithm is evidence based 2 and is stratified according to the Well’s score and a qualitative D-Dimer test (SimpliRed). Based on evidence 3, 4, 5 the use of a repeat Doppler ultrasound has largely replaced the venogram for those patients that have a negative doppler ultrasound and positive d-dimer. This study aims to audit this practice. Figure 2. Outcome of referrals for second ultrasound based on d-dimer result. Discussion Only 5.8% (95% CI 4.8 to 7.0) of patients with a negative ultrasound were referred for a second ultrasound, of which 6% (95% CI 2.8 to 12.5) were positive. None of those who had a negative d-dimer were diagnosed with DVT on a second ultrasound. However of those with a negative second ultrasound, 5.3% (95%CI 2.3 to 11.7) were subsequently diagnosed with DVT within 3 months. These cases amount to only 0.26% (95CI 0.11 to 0.60) of all those who had an ultrasound at the ED. Conclusion The use of a second ultrasound to diagnose DVT in patients with a negative first ultrasound is a useful strategy. However a small proportion of patients with negative second ultrasound were subsequently diagnosed with DVT. This needs further evaluation. Figure 1. Overview of referrals for second ultrasound. Results 1956 patients had a Doppler ultrasound. Of these 1720/1956 (87.9%; 95% CI 86.4 to 89.3) were negative.100/1720 (5.8%; 95% CI 4.8 to 7.0) were referred for second ultrasound. Outcome of second ultrasound referrals Of the 100 patients referred for a second ultrasound, 6/100 (6.0%; 95% CI 2.8 to 12.5) had a positive ultrasound. All 17 patients with a negative D-Dimer (100.0%; 95% CI 81.6 to 100.0) had a negative second ultrasound. Follow-up of negative second ultrasounds Over a 3 month period 5/94 (5.3%; 95% CI 2.3 to 11.7) patients who had a negative second ultrasound were subsequently diagnosed with DVT. These represent 5/1956 (0.26% 95CI 0.11 to 0.60) of all those who had an ultrasound at the ED. Methods Results of ultrasounds preformed over 12 months were collected from PACS and iSOFT databases. Patients who had a negative second ultrasound were followed up for subsequent diagnosis of DVT/PE for a period of 3 months. • References • Suspected Lower Limb Deep Vein Thrombosis Assessment Guideline. Department of Medicine / Department of A&E – Mater Dei Hospital. GDG July 2006 MED 01/Guide/2006/v01.1 • Wells PS et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management. Lancet. 1997 Dec 20-27;350(9094):1795-8. • Bernardi E, Camporese G, Buller HR, et al. Erasmus Study Group. Serial 2-point ultrasonography plus D-dimer vs whole-leg color-coded Doppler ultrasonography for diagnosing suspected symptomatic deep vein thrombosis: a randomized controlled trial. JAMA. 2008;300(14):1653-1659 • Kraaijenhagen RA et al. Simplification of the diagnostic management of suspected deep vein thrombosis. Arch Intern Med. 2002 Apr 22;162(8):907-11. • Righini M, Paris S, Le Gal G, Laroche JP, Perrier A, Bounameaux H. Clinical relevance of distal deep vein thrombosis: review of literature data. Thromb Haemost. 2006;95(1):56-64