Atopic Dermatitis
Atopic Dermatitis. Adam Goldstein, MD Associate Professor UNC Department of Family Medicine Chapel Hill, NC aog@med.unc.edu . Objectives. Improve ability to accurately diagnose and manage 90% of cases of atopic dermatitis

Atopic Dermatitis
E N D
Presentation Transcript
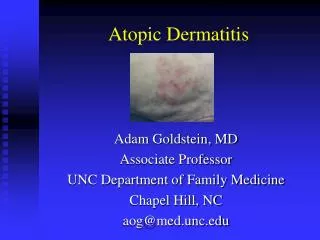
Atopic Dermatitis Adam Goldstein, MD Associate Professor UNC Department of Family Medicine Chapel Hill, NC aog@med.unc.edu
Objectives • Improve ability to accurately diagnose and manage 90% of cases of atopic dermatitis • Recognize differences in infant, childhood and adult presentations of atopic dermatitis • Improve ability to diagnose and manage conditions associated with and sometimes confused with atopic dermatitis
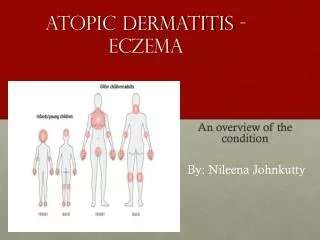
Atopic Dermatitis: Definition • Atopic dermatitis = eczema = itchy skin • Greek- meaning • (ec-) over • (-ze) out • (-ma) boiling • Infants & small children (affects 1 in 7) • Atopic dermatitis of childhood may reappear at different site later in life.
Atopic Dermatitis: Cause • The exact cause is unknown.
Atopic Dermatitis: Cause (Charlesworth, Am J Med, 2002)
Atopic Dermatitis: Cause • ? Inborn skin defect that tends to run in families, e.g. asthma or hay fever • 85% with high serum IgE and + skin tests food & inhalant (Jones, Clin Rev Allergy, 1993)
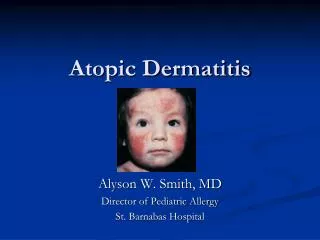
Distribution • In infants, the face is often affected first, then the hands and feet; dry red patches may appear all over the body. • In older children, the skin folds are most often affected, especially the elbow creases and behind the knees. • In adults, the face and hands are more likely to be involved.
Atopic Dermatitis: Associated features • The skin is usually dry, itchy & easily irritated by: • soap • detergents • wool clothing • May worsen in hot weather & emotional stress. • May worsen with exposure to dust & cats.
Associated Findings • Pityriasis alba
Associated Findings • Xerosis
Associated Findings • Keratosis Pilaris
Associated Findings • Ichthyosis
Diagnosis • Major characteristics • Pruritus with or without excoriation • Typical morphology and distribution • Chronic relapsing dermatitis • Personal or family history of atopy (asthma, allergy, atopic derm, contact urticaria) • Other characteristics • Xerosis/Ichthyosis/palmar hyper/kerat. pilaris • Early age of onset • Cutaneous colonization and/or overt infections • Hand/foot/nipple/contact dermatitis, cheilitis, conjunctivitis, Erythroderma, subcapsular cataracts (Drake, JAAD, 1992)
Differential Diagnosis • Seborrheic dermatitis
Differential Diagnosis • Seborrheic dermatitis • Scabies
Differential Diagnosis • Seborrheic dermatitis • Scabies • Drugs
Differential Diagnosis • Seborrheic dermatitis • Scabies • Drugs • Psoriasis
Differential Diagnosis • Seborrheic dermatitis • Scabies • Drugs • Psoriasis • Allergic contact dermatitis
Differential Diagnosis • Seborrheic dermatitis • Scabies • Drugs • Psoriasis • Allergic contact dermatitis • Cutaneous T-cell lymphoma
Atopic Dermatitis: Treatment 1. Reduce contact with irritants (soap substitutes) 2. Reduce exposure to allergens 3. Emollients 4. Topical Steroids 5. Antihistamines 6. Antibiotics 7. Steroid sparing 8. Other (herbals, soaps)
1. Reduce contact with irritants • Avoid overheating: lukewarm baths, 100% cotton clothes, & keep bedding to minimum • Avoid direct skin contact with rough fibers, particularly wool, & limit/eliminate detergents • Avoid dusty conditions & low humidity • Avoid cosmetics (make-ups, perfumes) as all can irritate • Avoid soap- use soap substitute • Use gloves to handle chemicals and detergents
Soap Substitutes • Cetaphil- soap substitute- far less drying and irritating than soap • Cleansing & moisturizing formulations, all OTC • Lotion, bar, ‘soap’, cream, sunscreen • Costs about $8-9 for 16 oz.
2. Reduce exposure to allergens • Keep home, especially bedroom, free of dust. • Allergic reactions include house dust mite, molds, grass pollens & animal dander. • Special diets will not help most individuals b/c little evidence that food is major culprit. • If food allergies exists, most likely d/t dairy products, eggs, wheat, nuts, shellfish, certain fruits or food additives.
3. Emollients • Emollients soften the skin soft and reduce itching. • Moisture Trapping effectiveness • Best:Oils (e.g. Petroleum Jelly) • Moderate: Creams • Least: Lotions • Apply emollients after bathing and times when the skin is unusually dry (e.g. winter months).
Emollients (cont’d) • Large variety (e.g. Vanicream, Eucerin, Lubriderm, Moisturel, Curel, Neutrogena) • Inexpensive emollients include vegetable shortening (Snowdrift by Martha White) and petroleum jelly (Vaseline) • Urea creams • Oils
Emollients: Alpha-Hydroxy acid • Creams are excellent for relieving dryness, but cansting & sometimes aggravate eczema • Useful for maintenance when no longer inflamed • Forces epidermal cells to produce keratin that is softer, more flexible and less likely to crack • Preparations • Glycolic Acid (8%) • Lactic Acid or Lac-Hydrin (5-12%) • Urea (3-6%) • Use 1X/ day
Emollients: Oils • Consider using bath oil or mineral oil-based lotions in lukewarm bath water • Add to tub 15 minutes into bath • Bath oil preparations: • Alpha-Keri • Aveeno bath • Jeri-Bath • Colloidal oatmeal (Aveeno) reduces itching
4. Corticosteroids • Topical steroids very effective • Ointments for dry or lichenified skin • Creams for weeping skin or body folds • Lotions or scalp applications for hair-areas.
Corticosteroids • Hydrocortisone 1-2.5% applied to all skin. • Quite safe used even for months • Use intermittently thin areas- (eg-face & genitals) • Stronger potency topical steroids for nonfacial/genital regions. • Avoid potent/ultrapotent topical steroid preparations on face, armpits, groins & bottom.
Corticosteroids • Once under control, intermittent use of topical corticosteroid may prevent relapse • Systemic steroids may bring under rapid control, but may precipitate rebound • Once daily probably most cost effective (Green, Br J Dermatol, 2005)
Steroids and Young Children • Fluticasone proprionate cream 0.05% • Moderate- severe atopic derm > 3 months • Applied bid 3-4 weeks- mean 64% BSA • No HPA suppression (Friedlander, J Am Acad Dermatol, 2002)
Corticosteroids: Pearls • Different preparations prescribed for different parts of body or for different situations • Educate on • potencies & proper usage • write down directions • Bring all topicals each appointment to clarify use
5. Antibiotics • Atopic eczema frequently secondarily colonized with a bacteria (up to 30%). • Use oral antibiotics in recalcitrant or widespread cases.
6. Antihistamines • Oral antihistamines can reduce urticaria & itch • Non-sedating antihistamines less side effects but more expensive • Sedative effect of hydroxyzine & diphenhydramine helpful
7. Steroid Sparing • Topical calcineurin inhibitors • Tacrolimus ointment & pimecrolimus cream • Oral Cyclosporine • Ultraviolet light therapy (phototherapy) with PUVA (psoralens plus ultraviolet A radiation) or combinations of UVA & UVB (Jekler, J Am Acad Dermatol, 1990)
Tacrolimus ointment (0.03%, 0.1% [Protopic]) • Mild to moderate eczema • Steroid dependent or signs of atrophy • Non-steroid responsive • BID x 2-4 weeks to evaluate response • Transient stinging possible • Longer disease-free intervals • Cost similar to high potency steroids (30gm/$60) (Ruzicka, N Engl J Med, 1997)
Pimecrolimus cream 1%(15, 30, 100 gm [Elidel]) • Approved Dec. 2001 • Blocks production/release cytokines T-cells • Moderate eczema • Steroid sparing • Transient stinging 8% children, 26% adults • Cost similar to high potency steroids (30gm/$60) (Ruzicka, N Engl J Med, 1997) (Eichenfield, J Am Acad Dermatol, 2002)