Shoulder Dystocia
Shoulder Dystocia. Or, The head’s out; what next? Ahmad Alkathiri MD. Objectives. At the completion of this presentation, the participant should be able to: Define shoulder dystocia (MK) Name three risk factors for shoulder dystocia (MK, PC)


Shoulder Dystocia
E N D
Presentation Transcript
Shoulder Dystocia Or, The head’s out; what next? Ahmad Alkathiri MD
Objectives • At the completion of this presentation, the participant should be able to: • Define shoulder dystocia (MK) • Name three risk factors for shoulder dystocia (MK, PC) • List potential complications, both maternal and fetal, of shoulder dystocia (MK) • Describe the maneuvers used to relieve a shoulder dystocia (MK, ICS)
Definition • “…a delivery that requires additional obstetric maneuvers following failure of gentle downward traction on the fetal head to effect delivery of the shoulders.” • ACOG, Practice Bulletin 40 (November 2002)
Definition • “Prolonged head-to-body expulsion time” • Objectively defined as 60 seconds • Deliveries with head-to-body interval of > 60 seconds more commonly have higher birth weight, shoulder dystocia, and low 1 minute Apgar scores • Beall et al 1998; Spong et al 1995
Functional Definition • A delivery in which the shoulders do not follow the head as usual, but rather are delayed in delivering or require the use of ancillary obstetric maneuvers to effect delivery. • The anterior shoulder may be impacted behind the symphysis pubis, or (less commonly) the posterior shoulder behind the sacral promontory
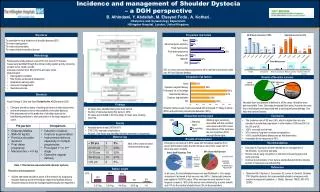
Incidence • Reported to occur in 0.2-2% of births • May recur with a higher frequency, but this is really unknown • Many women and clinicians will opt for cesarean in the future, especially if there has been a fetal injury • Recurrence rates reported 1-17%
Risk Factors • Maternal diabetes mellitus • Fetal macrosomia • Multiparity • Post-term pregnancy • Previous macrosomic infant • Previous shoulder dystocia
Macrosomia • Birth weight in excess of a specific weight, usually defined as either 4500 grams (1.5% of births) or 4000 grams (10% of births) • Birth weight > 4500 grams – rate of shoulder dystocia is 10-25% • Birth weight > 4500 grams AND maternal diabetes – rate of shoulder dystocia is 20-50%
Large for gestational age • Birth weight that exceeds the 90th centile of a standard growth curve, regardless of gestational age. • A baby may be LGA without being macrosomic
Pathophysiology • A “mismatch” between fetal size and maternal pelvic capacity • Positional variations – vertical rather than oblique orientation of shoulders • Increased diameter of shoulder girdle • Subcutaneous fat deposition may be increased in infant of diabetic mother – especially with sub-optimal glucose control
Anatomy of the Brachial Plexus • Nerve roots from C5-C8 and T1 • Merge into three trunks • Superior (C5, C6) • Middle (C7) • Inferior (C8, T1) • Each splits into anterior and posterior divisions
Anatomy of the Brachial Plexus • The six divisions regroup into three cords • Posterior – all 3 posterior trunk divisions (C5-T1) • Lateral – anterior divisions of upper and middle trunks (C5-C7) • Medial – continuation of lower trunk (C8, T1)
Brachial Plexus Injuries • Strain or stretch • Partial disruption • Complete avulsion
Brachial Plexus Injuries • Injury primarily to lateral trunk (C5,6, 7) leads to Erb’s palsy – adducted shoulder, extended elbow, and flexed wrist (“waiter’s tip”) • Injury primarily to the medial trunk (C8, T1) leads to Klumpke’s palsy – paralyzed hand with good shoulder and elbow function
Maternal Complications • Post-partum hemorrhage occurs in 11% • 4th degree laceration occurs in 3-4%
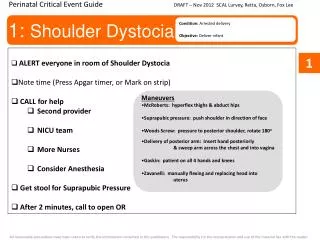
Clinical Management • Step One: Recognize the presence of a shoulder dystocia • Step Two: Be sure enough help is present • Nursing • Obstetrics • Pediatrics • Anesthesiology
Clinical Management • Step Three: Apply primary maneuvers • Mc Roberts maneuver • Oblique suprapubic pressure • Step Four: Apply secondary maneuvers; no prescribed order • Rubin; Woods screw; Posterior arm; All-fours; Clavicular fracture
Clinical Management • Step Five (concurrent): • Repeat steps three and four (different operator?) • Consider if an episiotomy is needed (intentional 4th degree?) • Step Six: Apply final (heroic) maneuvers • Zavanelli; symphysiotomy
Steps One and Two • The operator determines a shoulder dystocia is present • Personnel needed: • Nursing • At least two to assist with maneuvers • One to serve as “recorder”, as in a code 12 situation • Pediatrics – full resuscitation readiness
Steps One and Two • Personnel (continued) • Anesthesiology • Obstetrics • Attending to supervise and step in as needed • 2 residents at minimum • Ideally 2 at perineum • One to assist with maneuvers (suprapubic pressure) away from perineum
Step Three – Primary Maneuvers • McRoberts maneuver • Patient positioned with hips at edge of the broken-down birthing bed • Both hips are sharply flexed with knees remaining flexed (“knees to shoulders”) • Ideally performed by staff, not family, to assure it is adequately performed • No benefit to “prophylactic” McRoberts
McRoberts Maneuver • This maneuver assists delivery by: • Straightening maternal lumbar lordosis • Rotates symphysis superiorly and anteriorly • Improving angle between pelvic inlet and direction of maximal expulsive force • Elevates anterior shoulder allowing posterior shoulder to descend
Oblique suprapubic pressure • Usually applied in concert with McRoberts maneuver • Directed downward and laterally in order to effect rotation of the fetal anterior shoulder under the symphysis • Should be applied from the fetal posterior
Step Four – Secondary Maneuvers • There is no conclusive evidence that one maneuver is superior to another • In each patient, the operator must decide which maneuver will be most effective • This is a good time to decide about an episiotomy – is there room to get your hand in? • Time to initiate perinatal code (4-2012)
Woods screw maneuver • Apply pressure on the clavicle to effect rotation of the shoulders out of the vertical orientation • As fetus rotates, anterior shoulder should pass under symphysis • May be a good choice for a right-handed operator when the fetal occiput is oriented to the maternal right
Woods screw maneuver • Potential complication: • Fetal clavicular fracture IN DIRECTION OF APEX OF LUNG
Rubin’s maneuver • Apply pressure to the fetal scapula to effect rotation of the shoulders out of the vertical orientation • As fetus rotates, anterior shoulder should pass under symphysis • May be a good first choice for a right-handed operator when the fetal occiput is directed to the maternal left
Rubin’s maneuver • May result in need for less traction and less brachial plexus strain than McRoberts maneuver • Gurewitsch, 2005
Delivery of Posterior Arm • The operator inserts a hand into the vagina and locates the posterior arm. • The operator applies pressure in the antecubital fossa to flex the elbow across the chest • The operator grasps the forearm or hand and pulls it out of the vagina
Delivery of Posterior Arm • The anterior shoulder should pass under the symphysis • Rotation maneuvers (Woods or Rubin’s) can be applied if needed • This maneuver will tend to be more difficult with one’s non-dominant hand
Delivery of Posterior Arm • Potential complications • Fracture of humerus • Fracture of clavicle
Gaskin All Fours Maneuver • Attributed to midwife Ina May Gaskin • An option for a patient without anesthesia • Traction is applied in the opposite direction (still toward the floor, but now directed towards delivery of the posterior shoulder first)
Intentional clavicular fracture • Apply pressure over mid-clavicle in a vector AWAY from the lung • May be difficult to perform • If successful, may reduce the diameter of the shoulder girdle • Potential complication: • Lung injury
Still not out?! What now???
Step Five – Regroup and Repeat • Considerations: • Time passed so far? • Episiotomy? • Different operator? • Make OR preparations!
Step Six – Final Steps • Zavanelli maneuver (cephalic replacement) • Relax uterus with terbutaline • Rotate head back to OA (“reverse restitution”) • Flex neck • Upward pressure • To OR
Step Six – Final Steps • Symphysiotomy • Not commonly done when cesarean is available • Last ditch effort • Insert Foley catheter • Use vaginal hand to laterally displace urethra to avoid injury • Incise symphysis through mons pubis
Do not: • Panic • Apply any more lateral traction than would be applied in an uncomplicated delivery • Apply fundal pressure – may worsen the shoulder impaction or even rupture the uterus • Cut a nuchal cord until after the shoulders are released
Do: • Remain calm • Communicate well • Mark time of head delivery • Consider calling out time in one minute increments • Call for help • Document clearly and legibly
Do: • Be sure to “debrief” as a team after the delivery is completed • Opportunity to analyze situation and critique team performance • Opportunity to be sure documentation is consistent • Who did what becomes very important • Send cord gases
Do: • Review with the family exactly what happened and answer questions – soon after delivery, but probably not immediately • Follow the baby’s course in the nursery • Notify Risk Management