Download
1 / 31
420 likes | 924 Vues
MENSTRUAL DISORDERS. MELY K. By the end of this session the Learner will be able to: Define Normal menstruation Classify Menstrual Disorders Explain characteristics of the different menstrual disorders Demonstrate ability to diagnose menstrual disorders

E N D
MENSTRUAL DISORDERS MELY K.
By the end of this session the Learner will be able to: Define Normal menstruation Classify Menstrual Disorders Explain characteristics of the different menstrual disorders Demonstrate ability to diagnose menstrual disorders Apply Knowledge and skills acquired to manage menstrual disorders. Specific Objectives
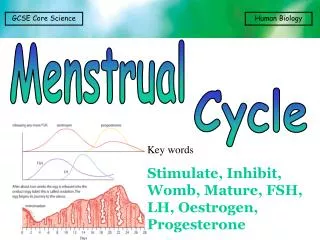
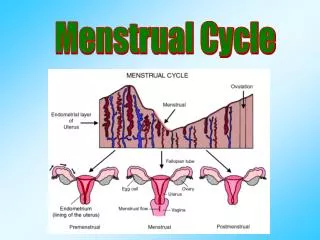
It is the cyclical shading of a functional endometrium; and has the following characteristics: Amount of flow: 25-80 ml average 30 mls Cycle length: 21-35 days Duration of flow: 2-7 days Healthy menstrual blood does NOT coagulate It occurs in a cyclic manner and regularly Definition of normal menstruation
Premenstrual syndrome (PMS) Mastodynia Abnormal bleeding due to gynecologic and non gynecologic disorders: Amenorrhea, oligomenorhea, hypomenorrhea, menorrhagia, polymenorrhea, metrorrhagia, etc Dysmenorrhoea Dysfunctional uterine bleeding (DUB) Post menopausal bleeding Classification of menstrual disorders
occurs in at least 3 consecutive menstrual cycles Symptoms must occur in the 2nd half of the menstrual cycle (luteal phase) There must be a symptom free period of at least 7 days in the 1st half of the cycle Symptoms must be severe enough to require medical advise or treatment e.g. oedema, weight gain, restlessness, irritability and increased tension. Premenstrual syndrome:
Symptoms include: Mood symptoms ( irritability, mood swings, depression, anxiety) Physical symptoms ( bloating, breast tenderness, insomnia, fatigue, hot flushes, appetite change, e.t.c) Cognitive changes (confusion and poor concentration) Premenstrual syndrome cont’d:
Mainly based on patient’s history Patient charts symptoms for at least 3 symptomatic cycles Rule out medical conditions that mimic PMS e.g. thyroid disease and anemia. PMS -Diagnosis
Diet: (limit caffeine, alcohol, tobacco and chocolate intake; eat small frequent meals Decrease sodium intake Stress management; Aerobic exercises Cognitive behavioral therapy PMS- Management( Conservative)
Calcium carbonate (for bloating, pain and food cravings) Magnesium ( for water retention) Vitamin B6 and vitamin E NSAIDs Bromocryptine for mastalgia PMS management(Drug therapy)
Also termed mastalgia Defined as: intolerable breast pain during the second half of the menstrual cycle. caused by edema and engorgement of the vascular and ductal systems Occurs cyclically in the luteal phase Mastodynia
History and examination Can be confirmed by aspiration Ultrasound Serial mammography Excisional biopsy sometimes is necessary Rule out: Mastitis, neoplasm Mastodynia -diagnosis
Breast support Avoid- coffee, tea, chocolate, cola drinks Avoid nicotine May occasionally use a mild diuretic Drug therapy: topical NSAIDS, Gosarelin (Zoladex), Limited success with: tamoxifen, danazol, bromocryptine, oral contraceptives, vitamins Mastodynia- treatment
Defined as excessive, heavy or prolonged menstrual flow Possible causes include: submucous myomas, adenomyosis, IUDs, endometrial hyperplasia, malignant tumors e.t.c Menorrhagia (Hypermenorrhea)
Defined as unusually light menstrual flow sometimes only spotting Possible causes include: hymenal or cervical stenosis, uterine synechiae (Asherman’s syndrome), occasionally oral contraceptives Hypomenorrhea (cryptomenorrhea)
Defined as bleeding occurring any time between the menstrual periods Possible causes include: endometrial polyps, CA cervix, CA endometrium, exogenous estrogen administration Metrorrhagia (intermenstrual bleeding)
Describes periods that occur too frequently Usually associated with anovulation and rarely with a shortened luteal phase in the menstrual cycle Polymenorrhea
This is bleeding that occurs at irregular intervals and varies in amount and duration of bleeding Caused by any condition that can lead to intermenstrual bleeding Menometrorhagia
Describes menstrual periods that occur more than 35 days apart Possible causes: anovulation which may be from endocrine causes (pregnancy, menopause, pituitary and hypothalamic disorders); or systemic causes (excessive weight loss); estrogen secreting tumors etc Oligomenorrhea
No menstrual period for more than 6 months Possible causes: Congenital uterine absence Hormonal disturbances from the hypothalamus and pituitary gland Failure of the ovary to receive or maintain egg cells Genetic diseases e.g. causes of intersex i.e. 5-alpha-reductase deficiency AMENORRHEA
History and physical examination Cytological examination –include biopsy and histology Pelvic ultrasound scan Endometrial biopsy Hysteroscopy Dilatation and curettage Hormonal profile Blood tests- Haemogram, thyroid function tests e.t.c. Diagnosis in abnormal uterine bleeding
Treat cause appropriately May include Hormonal preparations Surgery Endometrial ablation and endometrial resection, Prostaglandin synthetase inhibitors, Levonogestrel releasing IUDs Management of abnormal uterine bleeding- principles
Definition: Pain associated with menstruation Risk factors: Menstrual factors (early menarche, menorrhagia) Parity (lower in multipara) Diet (reduced intake of fish, eggs and fruits) Exercise (reduces dysmenorrhoea) Cigarette smoking (increases) Psychological (emotionally dependent and overprotected girls, family history,) Dysmenorrhea
Primary or spasmodic dysmenorrhea: Essential/ intrinsic / functional. Defined as painful menstruation in absence of pelvic pathology Usually starts at puberty Follows onset of ovulation and presents throughout period of bleeding. Congestive or secondary dysmenorrhea: Underlying pelvic disease e.g. uterine abnormalities, infections, endometriosis, foreign bodies, iatrogenic Membranous dysmenorrhea: associated with passage of endometrial cast through an undilated cervix. Dysmenorrhea- classification
Primary Dysmenorhea: Age: Usually seen among younger women Time of onset: 2-3 yrs after menarche Duration of pain: starts just prior to menses, lasts about 2 days Type of pain: cramping pain Membranous Dysmenorhea: Intense cramping pain associated with passage of an endometrial cast through an undilated cervix. Dysmenorhea- clinical features
Secondary Dysmenorhea: - Associated with specific diseases and disorders e.g. PID, Uterine fibroids, endometriosis etc Usually among older women (3rd to 4th decade) Time of onset: follows initial years of normal painless cycles Duration of pain: Onset is few days prior to menses and continues throughout cycle even after cessation of menses Type of pain: continuous dull aching or dragging pain Dysmenorhea- clinical features (ctd)
Dysmenorhea -management Dysmenorhea Assurance Laxatives Analgesics and Antispasmodics Fails Contraception not required or OC pills contraindicated Contraception required or NSAIDS contra indicated Prostaglandin synthetase inhibitors OC pills Fails Laparoscopy to look for causes of secondary Dysmenorhea No cause found but persistent and severe pain Cause found Treat as appropriate Surgery
Defined as a symptom complex that includes any condition of abnormal uterine bleeding in the absence of pathologic cause Commonly caused by anovulation as seen in polycystic ovarian disease and obesity May occur in all age groups from prepubertal girls to menopausal women Dysfunctional Uterine bleeding (DUB)
Medical management: NSAIDS Antifibrinolytic agents Hormones Surgical Endometrial resection Endometrial ablation hysterectomy DUB management
Any vaginal bleeding in a postmenopausal women should be considered abnormal Frequently associated with malignancies of the reproductive tract Benign causes include: endometrial /cervical polyps, trauma, senile vaginitis, vulval dystrophies Management depends on the cause. Postmenopausal bleeding