Menstrual Cycle
Menstrual Cycle. Fawaz Edris MD, FRCSC, FACOG, RDMS, AAACS Maternal Fetal Medicine Reproductive Endocrinology & Infertility. Introduction . Hypothalamus – Pituitary – Ovaries - Endometrium

Menstrual Cycle
E N D
Presentation Transcript
Menstrual Cycle Fawaz Edris MD, FRCSC, FACOG, RDMS, AAACS Maternal Fetal Medicine Reproductive Endocrinology & Infertility
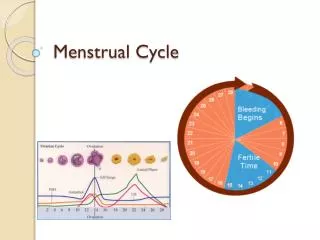
Introduction • Hypothalamus – Pituitary – Ovaries - Endometrium • Hormonal changes functional and morphological changes in ovaries ovulation endometrial changes implantation or menstruation • Hypothalamus – pituitary axis • Menstrual Cycle = Ovarian + Endometrial + Cervical + Vaginal + Breast + Psychological + Others
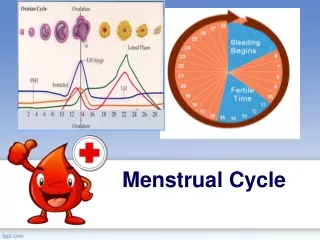
Ovarian Cycle • Estrogen. • Estrdiol (Ovary - Follicles) + Estrone (Androstendione – Aromatization) • Low in early proliferate phase • Rise 1 week before ovulation • Maximum 1 day before LH surge • Marked drop • Rise again to its maximum 5-7 days after ovulation (mid-luteal) • Baseline before menstruation
Ovarian Cycle • Progestins. • Progesterone (conversion from adrenal pregnenolone + pregnenolone sulphate) + 17-OHP • Minimal during follicular phase • Just before ovulation start to increase (from lutenized graafian follicle) – Hence need for LH/hCG during IVF • Rise to its maximum 5-7 days after ovulation (mid-luteal) – elevated BBT • Baseline before menstruation • If pregnancy continue
Ovarian Cycle • Androgens • Directly (small amount) from ovaries + adrenals • Indirectly (most amount) (metabolism from Androstenedione from ovaries & adrenals) • SHBG • Binds most Estrogens & Androgens • Prolactin • Levels do not change strikingly during cycle
Follicular Development • Primordial follicles (development – differentiation – maturation) • Mature graffian follicle(s) produced • Follicle rupture and release ovum • Ruptured follicle luteinize and produce corpus luteum
Follicular Development • During each cycle a cohort of follicles are recruited • One usually mature (18-25mm) – remain go into atresia • Mature follicle is estrogen dependent • Increase local FSH – continue to grow despite drop of mid-follicular FSH • FSH enhance FSH receptors increased E2 enhance FSH & LH receptors LH enhance androgen aromatization to E2 • LH receptors increase the response to mid-cycle LH surge which is important for final maturation, ovulation, and luteal progesterone production • Atresic follicles are androgen dependent • Decreased local FSH – cant grow • LH induced androgen will not aromatize and will lead to atresia
Ovulation • LH surge structural and biochemical changes to the growing follicle(s) • Dissolution of the entire follicular wall particularly at the surface of the ovary takes place (proteolytic enzymes) • Detachment (less attachment) of the oocyte along with the cumulus from the remain of the follicle • Oocyte adheres to the surface of the ovary for extended time allowing fallopian tube contractions to bring the ovary into close contact with the tubal epithelium • Tubal muscular contraction +/- tubal cilia movement contribute to the entry of & transportation of the ovum along the tube
Ovulation • At birth, primary oocyte are in the prophase of first meiotic division • Few hours before ovulation, meiotic division takes places, and secondary oocyte along with a polar body are produced (each 23 chromosomes) • After fertilization, second polar body is formed
Corpus Luteum • LH granulosa cells of ruptured follicle undergo luteinization • Luteinized granulosa cells + surrounding theca cells + capillaries + CT CL • CL ++++ progesterone & + E2 • Life span of CL = 9 - 10 days (unless pregnant) corpus albicans (avascular scar)
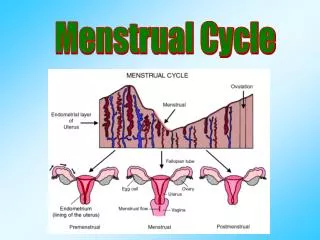
Endometrial Cycle • Endometrium is responsive to Progestins + Androgens + Estrogens menstruation & implantation & pregnancy • Functionally the endometrium is divided to 2 zones: • Outer portion (functionalis) • Cyclical changes in morphology & function during menstrual cycle • Sloughed off during menstruation • Occupied by spiral arteries (coiled) • Inner portion (basalis) • Relatively unchanged during menstrual cycle • Provide stem cells for the renewal of the funcionalis • Occupied by basal arteries (straight)
Endometrial Cycle • Histophysiology of the endometrium is divided into there stages: • Menstrual phase • Proliferative or estrogenic phase • Secretory or progestational phase
Menstrual Phase • First day of menstruation is day 1 of the cycle • Last 4-5 days • Disruption and disintegration of the endometrial glands & stroma • Leukocyte infiltration • RBC extravasaion • Sloughing of the funtionalis • Compression of the basalis • Renewed tissue growth within the basalis
Proliferative Phase • Endometrial proliferation or growth secondary to estrogenic stimulation • By the end of this stage: • Cellular proliferation & endometrial growth reached maximum • Numerous mitotic activity • Spiral arteries are elongated and convoluted • Endometrial glands are straight with narrow lumen containing glycogen
Secretory Phase • Following ovulation progesterone secretion by CL stimulates the glandular cells to produce glycogen, mucus, and others • Glands become tortuous and filled • Stroma become edematous • Mitosis are rare • Spiral arteries extend into superficial layer • If pregnancy doesn’t occur by day 23 • CL regress • Secretion of Progesterone and E2 decline • Endometrial involution • 1 day before menstruation, marked constriction of spiral arteriols takes place ischemia of endometrium lukocyte infiltration & RBC extravasation • Prostaglandin effects • Pain
Cervical Cycle • Although part of the uterus but different in many ways: • The mucosa does not undergo cyclical desquamation • Instead there are changes in the cervical mucus • Estrogen makes it thinner and alkaline • Thinnest at ovulation time (spinnbarkeit 8-12cm) • Promote sperm survival and transport • Progesterone makes it thicker and cellular • Histologically • Estrogen gives it fern like pattern • After ovulation & during pregnancy fail to fern
Vaginal Cycle • Estrogen • Cornified epithelium • Progesterone • Thick mucus secretion • Epithelial proliferation • Infiltration by leukocytes
Breast Cycle • Estrogen • Proliferation of the mammary ducts • Progesterone • Growth of lobules and alveoli • Distention of the ducts + hyperemia and edema of the interstitial breast tissue • Breast swelling, tenderness, and pain • Starts 10 days before menstruation and disappears with menstruation
Other Cyclical Changes • Temperature • Progesterone • Emotional • Psychological