Menstrual Cycle
Menstrual Cycle. Prepared by : Ayda khader. Feb.2017. The pituitary hormones Pituitary gland has two functional lobes: the anterior pituitary and posterior pituitary


Menstrual Cycle
E N D
Presentation Transcript
Menstrual Cycle Prepared by : Ayda khader Feb.2017
The pituitary hormones • Pituitary gland has two functional lobes: the anterior pituitary and posterior pituitary • The anterior pituitary produces 6 hormones under the influence of the releasing hormone of hypothalamus. Three of them are directly related to reproduction: • The follicle stimulating hormone (FSH): responsible for maturation of graffian follicle. • Luteinizing hormone (LH) brings at ovulation and the development of corpus luteum. • Prolactine: Initiate lactation.
The posterior pituitary gland produce two hormones: • Oxytocin: brings about contraction of smooth muscle fibers of reproductive tract and mammary cell during lactation • Vasopressin (ADH):Anti-diuretic hormone, which controls water balance and blood pressure
Pregnancy Hormones 1. Human Chorionic Gonadotrophin (HCG) hormone • Produced by cytotrophoblast (inner layer of the trophoblast) appears in the urine a few days after implementation of the ovum. • Serve functions as prolonging the life of corpus luteum during pregnancy and inhibit menstruation. 2. Human placental lactogen (HPL) • It is produced by syncytiotrophoblasts (outer layer of the trophoblast) that there concentration rises steeply during pregnancy until 36 weeks. • Assays of their serum are utilized as a measure of placental function
Steroids sex hormones 1. Estrogen • The estrogen hormone is produced under the influence of follicle stimulating hormones (FSH) of anterior pituitary gland. • Estrogens are produced primarily by Graffian follicles in the ovaries, the corpus luteum and the placenta. Luteinizing hormone (LH) stimulates the production of estrogen in the ovaries. Some estrogens are also produced in smaller amounts by other tissues such as the liver, adrenal glands, and the breasts.
2. Progesterone • Produced in early pregnancy by special glandular structure of the ovaries, corpus luteum (yellow body), under the influence of luteinizing hormone. • Later the placenta produces it in increasing quantities. • Involved in the female menstrual cycle (responsible for secretory phase) and pregnancy supports. • It plays no part in the secondary sexual characteristics which develop at puberty.
3. Testosterone • It’s a male steroid sex hormone that produced by interstitial cell of testes under the influence of LH. • Cause the development of adult male sex characteristics • Promote the growth and maturation of male reproductive system • In adulthood, testosterone is necessary for contentious production of sperm.
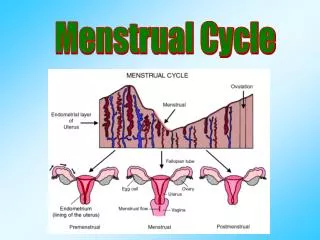
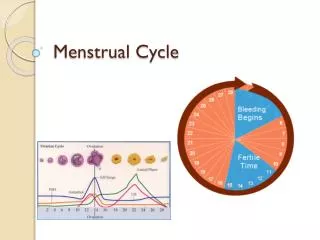
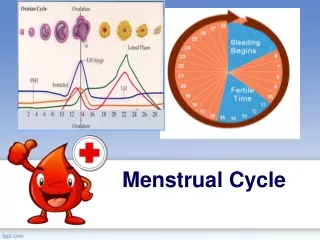
menstrual cycle • Menstrual cycle (also termed a female reproductive cycle) is a periodic uterine bleeding that begins with the shedding of secretoryendometrium approximately 14 days after ovulation. The purpose of menstrual cycle is to prepare the uterus for pregnancy. • The regularity of the menstrual cycle is controlled by the balance of four hormones: 1.Estrogens3. Follicle Stimulating Hormone 2.Progesteron (FSH) 4.Luteinizing Hormone (LH)
menstrual cycle • menstrual cycle is influenced by the ovarian cycle and endometrial cycle. 1. Ovarian Cycle The ovarian cycle pertains to the maturation of ova and consists of three phases 2. Endometrial Cycle The endometrial cycle pertains to the changes in the endometrium of the uterus in responses to the hormonal changes that occur during the ovarian cycle. This cycle consist of three phases.
Ovarian Cycle 1. Follicular or Preovulatory Phase (Days 5-13: Estrogen is Secreted, FSH Falls) • This phase is also called the proliferative phase because a hormone causes the lining of the uterus to grow, or proliferate during this time • A large amount of estrogen is secreted by the follicle during this phase of the menstrual cycle. • FSH controls the growth and maturity of graafian follicles. • Graafian follicles begin to secrete estrogen. • LH continue to rise slowly. • FSH begins to decrease in late follicular phase due to rising of estrogen,.
This estrogen does several things: 1. The estrogen stimulates the endometrial lining of the uterus. It becomes thicker and enriched. 2. One follicle begins to ripen and brings an egg to maturity 3. The estrogen suppresses the further secretion of FSH
2. Day 14: Ovulation Phase (Day 14) • At about mid-cycle, the estrogen helps stimulated a large and sudden release of luteinizing hormone (LH). This LH Surge, which is accompanied by a transient rise in body temperature, is a sign that ovulation is about to happen • The LH surge causes the follicle to rupture and expel the ripened egg into the fallopian tube.
3. Luteal (Days 15-28: Secretory Phase) Estrogen and Progesterone Secretion Rise, decrease of FSH, LH • After the follicle is ruptured, its walls collapse. It is now known as the corpus luteum. • Immediately after ovulation, the corpus luteum begins secreting large amounts of progesterone, which helps prepare the endometrial lining for implantation of the fertilized egg. • If the egg is fertilized, a small amount of the hormone called human chorionic gonadotrophin (HCG) is released
Levels of LH and FSH falls because of increase levels of estrogen and progesterone production from corpus luteum • If the egg is not fertilized, the corpus luteum starts to "crumble", causing the levels of estrogen and progesterone to drop. Without these hormones to support it, the uterus soon sheds its lining, and menstruation begins • In addition, with no estrogen to suppress it, FSH levels again start to rise. Thus, one cycle ends and another begins.
Endometrial Cycle 1.Menstrual or Bleeding Phase (Days 1-5: Estrogen Falls, in the last phase FSH Rises) Menstrual bleeding begins on Day 1 of the cycle and lasts approximately 3-5 days. During the last few days prior to Day 1, a sharp falls in the levels of estrogen and progesterone signals the uterus that pregnancy has not occurred during this cycle. This signal results in a shedding of the endometrial lining of the uterus. Since high levels of estrogen suppress the secretion of FSH, the drop in estrogen now permits the level of FSH to rise. FSH stimulates follicle development.
By Day 5 to 7 of the cycle, one of these follicles responds to FSH stimulation more than the others and becomes dominant. • As it does so, it begins secreting large amounts of estrogen
2. The proliferative phase: • Occurs following menstruation and ends with ovulation. During this phase, the endometrium is preparing for implantation by becoming thicker and more vascular. • These changes are in response to the increasing levels of estrogen produced by the graafian follicle.
3. The secretory phase: • Begins after ovulation and ends with the onset of menstruation. During this phase, the endometrium continues to thicken. The primary hormone during this phase is progesterone which is secreted from the corpus luteum. • If pregnancy occurs, the endometrium continues to develop and begins to secrete glycogen. • If pregnancy does not occur and the corpus luteum begins to degenerate and the endometrial tissue degenerates.
Menstrual Disorder 1. Dysmenorrhea Painful menstruation that interferes with daily activities. The possible cause is increased production of endometrial prostaglandin. It has two types: • Primary dysmenorrhea • secondrydysmenorrhea
Primary Dysmenorrhea • Occurs in the absence of organic diseases • Usually appears throughout the first 2-3 years after menarche • Its often improve by age or following pregnancy • Symptoms may include pain in the back, thighs, uterine cramp and GI upset as anorexia, nausea and vomiting. And the last for 1 to 3 days.
Secondary Dysmenorrhea Occurs in association with pathological changes such as endometriosis, • pelvic inflammatory disease, • cervical stenosis, uterine or ovarian neoplasm or uterine polyps • Presence of IUD may lead to secondary dysmenorrhea
Management: • Mild analgesia • Prostaglandin inhibitors (NSAID). • Contraceptives may be used • Regular exercise • Emotional support
Premenstrual Syndrome (PMS) • Is condition related to neuroendocrine events with the hypothalamic pituitary axis that modulate neurotransmitter function. • It has a relation with luteal phase and differs from dysmenorrhea in that it has no relation to ovulation. • Causes unclear but it may be due to hereditary or environmental factors.
Clinical manifestations Symptoms may begin 10 days or more prior to menstrual flow onset. they diminish 1 to 2 days after menses begin. It includes transitory edema, breast swelling and abdominal distension due to increase water content tissues, behavioral problems include irritability, sleep disturbances, depression, headache and vertigo. Management • Progesterone supplement • Diuretices. • Tranqulizers may be helpful • Low sodium diet.
Amenorrhea Absence of menstrual flow, It has two types: I. Primary Amenorrhea • A girl 16 years and has not menstruated yet. • Caused by congenital obstruction. Congenital absence of uterus and absence or imbalance of hormones II. Secondary Amenorrhea • A girl menstruation has begun but stops. • Physiological conditions as pregnancy, lactation and use of contraceptive • Pathological condition as hormonal imbalance, poor nutrition, ovarian lesion and stress.
III. Post pill amenorrhea after discontinuing oral contraception, there is usually a delay before ovulation and menstrual cycle recur. • However, amenorrhea exceeding 6 months should be investigated. Treatment: according to the cause.
Oligomenorrhea • The term oligomenorrhea refers to infrequent menstruation (decrease in time) or in occasional usage very light bleeding (decrease in amount). • There are several symptoms: less than nine periods in a year, unpredictable periods, difficulty conceiving and periods that are more than 35 days apart
Menorrhagia Menorrhagia is an abnormally heavy or prolonged menstrual period at regular intervals. Treatment options depend upon the cause of the condition. NSAIDs and contraceptive pills may relieve the symptoms
Metrorrhagia • Metrorrhagia or intermenstrual bleeding refers to any episode of bleeding that occurs between the expected regular menstrual periods. • It’s significant because usually a symptoms of other diseases as cancerous or benign tumor of uterus, endometriosis and uterine fibroids. • Mittlestaining, small of bleeding or spotting occurs at the time of ovulation.
Polymenorrhea • Polymenorrhea occurs when the menstrual cycle is less than 21 days long. • It is sometimes difficult to distinguish polymenorrhea from metrorrhagia; however, bleeding that occurs at regular intervals less than 21 days apart is usually polymenorrhea.
Menopause • Is the stage of female life when there is physiologic cessation of the menses along with progressive ovarian failure. Climacteric is the transition period during which the woman's reproductive function gradually diminishes and disappears. It usually occurs between the age of 45 and 55 years • Menopause can be surgically induced • The age of onset may be influenced be nutritional, cultural, and genetic factors. • Menopause occurs when estrogen levels come so low.
50% of women report symptoms of heat (hot flashes) arising on the chest and spreading to the neck and face caused be vasodilatation and last for 20-30 days • Long range physical changes may include osteoporosis. • Reproductive female system starts to atrophy. • Menopausal women may need assistance in the form of counseling to adjust successfully to this developmental stage of life. The way of dealing depends on socio-cultural factors and acceptance to menopause woman.