Download
1 / 61
610 likes | 807 Vues
Medical biology, microbiology, virology, immunology department. HYPERSENSITIVITY. TRANSPLANTATION AND TUMOR IMMUNITY. By as. E.V. Pokryshko. HYPERSENSITIVITY (ALLERGY)

E N D
Medical biology, microbiology, virology, immunology department HYPERSENSITIVITY. TRANSPLANTATION AND TUMOR IMMUNITY By as. E.V. Pokryshko
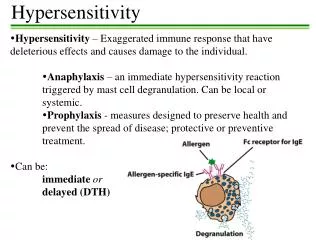
HYPERSENSITIVITY (ALLERGY) When an immune response results in exaggerated or inappropriate reactions harmful to the host, the term hypersensitivity,or allergy,is used. The clinical manifestations of these reactions are typical in a given individual and occur on contact with the specific antigen (allergen) to which the individual is hypersensitive.
Allergens are subdivided into • household and epidermal (the dust of feather quilts and pillows, skin epidermis, dandruff of dogs, cats, and horses, etc.), • occupational (library dust, dust of wool and cotton, certain dyes, soaps, varnishes, wood pulp, explosives and synthetic substances, etc.), • plant (the pollen of plants during pollination of meadow grasses, garden and potted plants), • food (eggs, strawberries, shellfish, citrus fruits, coffee, chocolate, and other foods), • drug (codeine, acetylsalicylic acid, sulphanilamides, penicillin and other antibiotics).
The activity of allergens is determined by their structure and the position of the determinant groups in their molecules. The allergens are of bacterial and fungal origin, protein-polysaccharide-lipid complexes. Different allergens have antigenic determinants in common (polyvalent character of allergic reactions).
Peter Gell and Robert Coombs developed a classification system for reactions responsible for hypersensitivities in 1963. Their system correlates clinical symptoms with information about immunologic events that occur during hypersensitivity reaction. The Gell-Coombs clasification system divides hypersensitivity into four types: Type I (Anaphylaxis) Hypersensitivity Type II (Cytotoxic) Hypersensitivity Type III (Immune Complex) Hypersensitivity Type IV (Cell-Mediated) Hypersensitivity
Allergic reactions • are subdivided into two groups: • immediate, • delayed reactions. • Although it is difficult to draw a strict distinction between them. • Allergic reactions ofimmediate actionare associated with B-lymphocytes and antibodies circulating in the blood, allergic reactions ofdelayed action with T-lymphocytes.
TYPE I: IMMEDIATE HYPERSENSITIVITY (ANAPHYLACTIC) An immediate hypersensitivity reaction occurs when antigen binds to IgE on the surface of mast cells with the consequent release of several mediators. The process begins when an antigen induces the formation of IgE antibody, which binds firmly by its Fc portion to basophils and mast cells. Reexposure to the same antigen results in cross-linking of the cell-bound IgE and release of pharmacologically active mediators within minutes (immediate reaction). Cyclic nucleotides and calcium play essential roles in release of the mediators.
No single mediator accounts for all the manifestations of type I hypersensitivity reactions. Some important mediators and their effects are as follows: (1) Histamine occurs in granules, of tissue mast cells and basophils in a preformed state. Its release causes vasodilation, increased capillary permeability, and smooth-muscle contraction. Clinically, disorders such as allergic rhinitis (hay fever), urticaria, and angioedema can occur. The bronchospasm so prominent in acute anaphylaxis results, in part, from histamine release. (2) Slow-reacting substance of anaphylaxis (SRS-A) consists of several leukotrienes, which do not exist in a preformed state but are produced during anaphylactic reactions. Leukotrienes are formed from arachidonic acid by the lipoxygenase pathway and cause increased vascular permeability and smooth-muscle contraction.
(3) Eosinophil chemotactic factor of anaphylaxis (ECF-A) (4) Serotonin is preformed in mast cells and blood platelets. When released during anaphylaxis, it causes capillary dilation, increased vascular permeability, and smooth-muscle contraction (5) Prostaglandins and thromboxanes are related to leukotrienes. Prostaglandins cause dilation and increased permeability of capilaries and bronchoconstriction. Thromboxanes aggregate platelets.
Atopy. Atopic disorders, such as hay fever, asthma, eczema, and urticaria, are immediate-hypersensitivity reactions that exhibit a strong familial predisposition and are associated with elevated IgE levels. Several processes seem likely to play a role in atopy, for example, failure of regulation at the T cell level (eg, increased production of interleukin-4 leads to increased IgE synthesis), enhanced uptake and presentation of environmental antigens, and hyperreactivity of target tissues. It is estimated that up to 40% of people in the United Stales have experienced an atopic disorder at some time in their lives. The symptoms of these atopic disorders are induced by exposure to the specific allergens. These antigens are typically found in the environment (eg, pollens and dust mite feces often found in bedding and carpet) or in foods (eg, shellfish and nuts).
Skin testing can be used for identify the allergen responsible for allergies. These tests involve inoculating small amounts of suspect allergen into the skin. Sensitivity to the allergen is shown by a rapid inflammatory reaction characterizide by redness, swelling, and itching at the site of inoculation
DesensitizationMajor manifestations of anaphylaxis occur when large amounts of mediators are suddenly released as a result of a massive dose of antigen abruptly combining with IgE on many mast cells. This is systemic anaphylaxis, which is potentially fatal. Desensitization can prevent systemic anaphylaxis.
H2 blockers inhibiting allergic response. Antigens (green triangles) enter the body, bind with IgE on mast cells (middle left), and trigger the release of histamine (green balls). Histamine attaches to receptors on blood vessels, causing vasodilation, edema, and inflammation. H2 blocker drugs (yellow balls) block histamine from engaging the receptors.
Acute desensitizationinvolves the administration of very small amounts of antigen at 15-minute intervals. Antigen-IgE complexes form on a small scale, and not enough mediator is released to produce a major reaction. This permits the administration of a drug or foreign protein to a hypersensitive person, but hypersensitivity is restored days or weeks later.
Chronic desensitizationinvolves the long-term weekly administration of the antigen to which the person is hypersensitive. This stimulates the production of IgG-blocking antibodies in the serum, which can prevent subsequent antigen from reaching IgE on mast cells, thus preventing a reaction.
TYPE II: CYTOTOXIC HYPERSENSITIVITY Cytotoxic hypersensitivity occurs when antibody directed al antigens of the cell membrane activates complement. This generates a membrane attack complex, which damages the cell membrane. The antibody (IgG or IgM) attaches to the antigen via its Fab region and acts as a bridge to complement via its Fc region. As a result, there is complement-mediated lysis as in hemolytic anemias, ABO transfusion reactions, or Rh hemolytic disease. In addition to causing lysis, complement activation attracts phagocytes to the site, with consequent release of enzymes that damage cell membranes.
Drugs (eg, penicillins, phenacetin, quinidine) can attach to surface proteins on red blood cells and initiate antibody formation. Suchautoimmune antibodies (IgG) then interact with the red blood cell surface and result is hemolysis. Certain infections, eg, Mycoplasma paeumoniae infection, can induce antibodies that cross-react with red cell antigens, resulting in hemolytic anemia.
In rheumatic fever, antibodies against the group A streptococci cross-react with cardiac tissue. Other drugs can attach to platelets and induce autoantibodies that lyse the platelets, producing thrombocytopenia and, as a consequence, a bleeding tendency. Others (eg, hydralazine) may modify host tissue and induce the production of autoantibodies directed at cell DNA. As a result, disease manifestations resembling those of systemic lupus erythematosus occur. In Goodpasture's syndrome, antibody to basement membranes of the kidneys and lungs bind to those membranes and activate complement.
TYPE III: IMMUNE-COMPLEX HYPERSENSITIVITY occurs when antigen-antibody complexes induce an inflammatory response in tissues. Normally, immune complexes are promptly removed by the retticuloendothelial system, but occasionally they persist and are deposited in tissues, resulting in several disorders. In persistent microbial or viral infections, immune complexes may be deposited in organs, eg, the kidneys, resulting in damage. In autoimmune disorders, "self antigens may elicit antibodies that bind to organ antigens or deposit in organs as complexes, especially in joints (arthritis), kidneys (nephritis), or blood vessels (vasculitis).
Wherever immune complexes are deposited, they activate the complement system. Polymorphonuclear cells are attracted to the site, and inflammation and tissue injury occur.
Two typical type III hypersensitivity reactions are • the Arthus reaction • serum sickness. Arthus Reactionis the name given to the inflammation caused by the deposition of immune complexes at a localized site. It is named for Arthus, who first described the inflammatory, response that occurs under the following conditions. If animals are given an antigen repeatedly until they have high levels of IgG antibody and that antigen is then injected subcutaneously or intradermally, intense edema and hemorrhage develop, reaching a peak in 3-6 hours. Antigen, antibody, and complement are deposited in vessel walls; polymorphonuclear cell infiltration inlravascular clumping or platelets then occur. These reactions can lead to vascular occlusion and necrosis. A clinical manifestation of the Arthus reaction is hypersensitivity pneumonitis (allergic alveolitis) associated with the inhalation of thermophilic actinomycetes ("farmer's lung").
Serum Sickness.In contrast to the Arthus reaction, which is localized inflammation, serum sickness is a systemic inflammatory response to the presence of immune complexes deposited in many areas of the body. After the injection of foreign serum (or, more commonly these days, certain drugs), the antigen is excreted slowly. During this time, antibody production starts. The simultaneous presence of antigen and antibody leads to the formation of immune complexes, which may circulate or be deposited at various sites. Typical serum sickness results in fever, urticaria, arthralgia. lymphadenopathy, splenomegaly, and eosinophilia a few days to 2 weeks after injection of the foreign serum or drug.
Immune-Complex Diseases A. Glotnerulonephritis:Acute poststreptococcal glomerulonephritis is a well-accepted immune-complex disease. B. Rheumatoid Arthritis:Rheumatoid arthritis is a chronic inflammatory autoimmune disease of the joints seen commonly in young women. C. Systemic Lupus Erythematosus:is a chronic inflammatory autoimmune disease that affects several organs, especially the skin of the face, the joints, and the kidneys.
TYPE IV: DELAYED (CELL-MEDIATED) HYPERSENSITIVITY • is a function of T lymphocytes, not antibody.It can be transferred by immunologically committed (sensitized) T cells, not by serum. The response is "delayed"; ie, it starts hours (or days) after contact with the antigen and often lasts for days. • In certain contact hypersensitivities, such as poison oak, the pruritic, vesicular skin rash is caused by CD-8-positive cytotoxic T cells that attack skin cells that display the plant oil as a foreign antigen. • In the tuberculin skin test, the indurated skin rash is caused by CD-4-positive helper T cells and macrophages that are attracted to the injection site.
TYPE IV: DELAYED (CELL-MEDIATED) HYPERSENSITIVITY The sensitized lymphocytes carry on their surface receptors which are antideterminants, specific to the given antigen. They bind with the foreign antigen by means of these receptors and destroy it with their enzymes and by producing special humoral factors, lymphokinins, which act as auxiliary vehicles of cellular immunity. Some types of lymphokinins may mobilize non-immune lymphocytes and include them in the reactions of cellular immunity.
Contact Hypersensitivity:This manifestation of cell-mediated hyper- sensitivity occurs after sensitization with simple chemicals (eg, nickel, formaldehyde), plant materials (eg, poison ivy, poison oak), topically applied drugs (eg, sulfonamides, neomycin), some cosmetics, soaps, and other substances. In all cases, the small molecules acting as haptens enter the skin, attach to body proteins, and become complete antigens.Cell-mediated hypersensitivity is induced, particularly in the skin.
Upon a later skin contact with the offending agent, the sensitized per- son develops erythema, itching, vesicles, eczema, or necrosis of skin within 12-48 hours. Tuberculin-Type Hypersensitivity:Delayed hypersensitivity to antigens of microorganisms occurs in many infectious diseases and has been used as an aid in diagnosis. It is typified by the tuberculin reaction. When a patient previously exposed to Mycobacterium tuberculosis is injected with a small amount of tuberculin (PPD) intradermally, there is little reaction in the first few hours. Gradually, however, induration and redness develop and reach a peak in 48-72 hours. A positive skin test indicates that the person has been infected with the agent, but it does notconfirm the presence of current disease. However, if the skin test converts from negative to positive, it suggests that the patient has been recently infected. Cell-mediated hypersensitivity develops in many bacterial, viral, protozoan and helminthic infections. A positive skin test response assists in diagnosis and provides support for chemoprophylaxis or chemotherapy.
Tuberculin (allergic) testsare used for detecting infection of children with M. tuberculosis and for determining infection with M. tuberculosis. Skin test
ALLERGY DIAGNOSTIC TESTS. Many infectious diseases are associated with the development of the body's elevated sensitivity toward the causative agents and products of their metabolism. Allergy tests used for the diagnosis of bacterial, viral, and protozoal infections, as well as mycosis and helminthiasis, rely exactly on this phenomenon. Allergy tests are quite specific but not infrequently they can be observed in vaccinated individuals and in those with a history of the disease in question.
All allergy tests are divided into two groups, namely, in vivo and in vitro tests. The first group (in vivo) consists of cutaneous tests made directly on the patient and revealing allergy of immediate (in 20 min) or delayed (in 24-48 hrs) type. Cutaneous Tests.Infective allergens are most often administered either intracutaneously or epidermally by rubbing them into scarified sites of the skin, less commonly they are injected subcutaneously.
In Vitro Tests.These methods of investigation are safe for the patient, highly sensitive, and allow to carry out a quantitative assessment of the body's allergization. To date, a number of tests have become available in which reactions with T- and B-lymphocytes, tissue basophils, neutrophil granulocytes, etc. are employed for this purpose. These tests include inhibition of leucocyte migration and lymphocyte blast transformation, specific rosette formation, the parameter of neutrophil granulocyte damage, Shelley's basophil test, reaction of tissue basophil degranulation. Still another test involves determination of IgE in blood serum.
TRANSPLANTATION An autograft(transfer of an individual's own tissue to another site in the body) is always permaently accepted, ie, it always "takes". A syngeneic graftis a transfer of tissue between genetically identical individuals, ie, identical twins, and almost always "takes" permanently. A xenograft, a transfer of tissue between-different species, is always rejected by an immunocom- petent recipient. An allograftis a graft between genetically different members of the same species, eg, from one human to another.