Understanding Type I Hypersensitivity Reactions: An Overview
Learn about Type I hypersensitivity reactions, an exaggerated immune response to antigens leading to damage. Explore the mechanisms, clinical manifestations, and genetic predispositions associated with this hypersensitivity type.


Understanding Type I Hypersensitivity Reactions: An Overview
E N D
Presentation Transcript
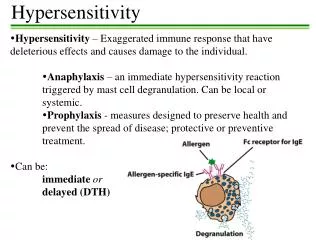
Hypersensitivity • Excessive response to antigen • Exaggerated immune response • Response to antigens leading to damage
Four Types of Hypersensitivity Reactions: • Type I (Anaphylactic) • Type II (Antibody-mediated/Cytotoxic) • Type III (Immune Complex) • Type IV (Cell-Mediated) – delayed hypersensitivity
Type I • An excessive response to antigens(allergens) leading to damage • Require sensitizing dose(s) • Both exogenous & endogenous antigens • Dust, pollens, foods, drugs, microbes, chemicals, blood products…. • Itching of the skin, to potentially fatal diseases – bronchial asthma, anaphylaxis
Type I • Sensitized host • IgE antibody - previously bound to the surface of mast cells & basophils • Interaction of allergen with IgEantibody • A response that occurs rapidly (within minutes)
Type I • Antigens are called “allergens” • Unknown why people get allergies, • Strong genetic predisposition (called atopy)
Type I Hallmark - inappropriate production of IgE against allergens that cause mast cell degranulation and release several mediators
Mast Cell - releases inflammatory mediators - increases vascular permeability
Basophils • similar to mast cells in many respects • not present in tissues. • they circulate - in the blood in extremely small numbers (0-1%) • can be recruited to inflammatory sites.
Type I • The allergen stimulates the induction of CD4+ T cells of the TH2 type. • CD4+ cells play a pivotal role in the pathogenesis of type I hypersensitivity • The cytokines secreted by them (IL-4, IL-5) cause IgE production by B cells, • IL-4, IL-5 act as growth factors for mast cells; recruit & activate eosinophils.
Type I • IgE antibodies bind to receptors expressed on mast cells & basophils; • Once the mast cells/basophils are thus "armed," the individual is primed to develop type I hypersensitivity. • Re-exposure to the same antigen results in cross-linking of the cell-bound IgE • Triggers a cascade of intracellular signals leading to the release of several powerful mediators.
Mast cell degranulation • Histamine: - Dilates & increases permeability of blood vessels (swelling & redness), - increases mucus secretion (runny nose), - smooth muscle contraction (bronchospasm). • Prostaglandins: -bronchospasm - increased mucus secretion. • Leukotrienes:bronchospasm
Type I • Two well-defined phases: (1) the initial response, • characterized by vasodilation, vascular leakage, smooth muscle spasm, • usually evident within 5 to 30 minutes after exposure to an allergen • subsiding by 60 minutes;
Type I (2) late-phase reaction starts in 2 to 8 hours lasts for several days. • characterized by more intense infiltration of tissues with eosinophils • tissue destruction in the form of mucosal epithelial cell damage.
Clinical manifestationsSystemic anaphylaxis Systemic (parenteral) administration of protein antigens or drugs (e.g., bee venom or penicillin) Within minutes of exposure in a sensitized host, itching, urticaria (hives), & skin erythema appear, • followed in short order by profound respiratory difficulty caused by pulmonary bronchoconstriction & hypersecretion of mucus.
Clinical manifestationsSystemic anaphylaxis • Laryngeal edema may exacerbate matters by causing upper airway obstruction. • GI & bladder smooth muscle contraction • The musculature of the entire GIT may be affected, with resultant • vomiting, abdominal cramps, diarrhea. • shock & death within minutes if untreated
Localised anaphylaxis • Allergic rhinitis (hay fever) • Asthma • Food allergies • Atopic Dermatitis (allergic eczema)
Localised anaphylaxis • Susceptibility to localized type I reactions appears to be genetically controlled( atopy ) • Patients who suffer from nasobronchial allergy (hay fever & some forms of asthma) often have a family history.
Allergic rhinitis (hay fever) • Inhaled allergen triggers reaction in nasal mucosa • Watery exudate from nose, eyes, upper respiratory tract, sneeezing, coughing
Asthma • Extrinsic asthma – due to inhaled airborne allergens (pollens, dust, fumes, etc) • Asthma may be triggered by cold, exercise • Bronchoconstriction, airway edema, mucus secretion, inflammation
Food allergies • Ingestion of allergen • Vomiting, diarrhea • If allergens are absorbed into bloodstream, reactions can occur where allergen deposits • Asthma-like symptoms • Urticaria (hives, wheal & flare response)
Atopic Dermatitis (allergic eczema) • Often occurs in young children • Red skin rash • Strong hereditary predisposition
Type I • Skin testing • Potential allergens are injected or scratched into the skin • If the patient is allergic a wheal & flare response occurs
TYPE II - IgG or IgM mediated • Complement involved • Complement activation causes cell lysis or damage by macrophages (phagocytosis)
Type II Antibodies (IgM or IgG) bind to cell surface antigens. • Antigen/antibody complex may lead to: • Complement activation lysis • Opsonization phagocytosis • Antibody-dependent cell-mediated cytotoxicity (ADCC), • These are normal reactions, but when they cause unwarranted tissue damage, they are considered a hypersensitivity.
Type II • Mediated by antibodies directed against target antigens on the surface of cells or other tissue components. • The antigens may be normal molecules intrinsic to cell membranes or extracellular matrix, or adsorbed exogenous antigens (a drug metabolite).
COMPLEMENT-DEPENDENT REACTIONS • Complement can mediate cytotoxicity via two mechanisms: Direct lysis Opsonization & phagocytosis • Antibody bound to a cell surface antigen causes fixation of complement with subsequent lysis via the membrane attack complex (MAC) • Cells coated with antibodies & C3b (opsonin) are also susceptible to phagocytosis
Complement ATTACK! • C3b serves an opsonin function • Some C3b binds to C4bC2a to form the C5 convertase (C4bC2aC3b) • C5 convertase cleaves C5 leading to the formation of the Membrane Attack Complex – MAC (C5-C6-C7-C8-C9) • The MAC “punches holes” in cell walls resulting in lysis
ANTIBODY-DEPENDENT CELL-MEDIATEDCYTOTOXICITY (ADCC) • This form of antibody-mediated injury involves killing via cell types that bear receptors for the Fc portion of IgG; targets coated by antibody are lysed without phagocytosis or complement fixation. • ADCC may be mediated by a variety of leukocytes - neutrophils, eosinophils, macrophages, and NK cells.
Although ADCC is typically mediated by IgG antibodies, in certain instances (e.g., eosinophil-mediated killing of parasites) IgE antibodies are used.
Clinically, antibody-mediated reactions occur in the following situations: • Transfusion reactions, where red cells from an incompatible donor are destroyed after being coated with recipient antibodies directed against the donor's blood group antigens. • Erythroblastosis fetalis due to rhesus antigen incompatibility; maternal antibodies against Rh in a sensitized Rh negative mother cross the placenta & cause destruction of Rh-positive fetal red cells.
Autoimmune hemolytic anemia, agranulocytosis, or thrombocytopenia resulting from an individual's generating antibodies to his or her own blood cells. • Drug reactions, where antibody is directed against a particular drug (or its metabolite) that is nonspecifically adsorbed to a cell surface (hemolysis that can occur after penicillin administration).
Complement mediated inflammation • Recruits WBC • Release enzymes, free radicals Eg: Good-pasture syndrome Vascular rejection in organ grafts
ANTIBODY-MEDIATED CELLULARDYSFUNCTION • antibodies directed against cell surface receptors impair or dysregulate function without causing cell injury or inflammation.
ANTIBODY-MEDIATED CELLULARDYSFUNCTION • Myasthenia Gravis antibodies against acetylcholine receptors in the motor end-plates of skeletal muscles impair neuromuscular transmission with resultant muscle weakness.
ANTIBODY-MEDIATED CELLULARDYSFUNCTION Conversely, antibodies can stimulate cell function. • In Graves disease, antibodies against the thyroid-stimulating hormone (TSH) receptor stimulate thyroid epithelial cells result in hyperthyroidism