Hypersensitivity Reactions: Types, Manifestations, & Treatment
Learn about hypersensitivity reactions, including Coombs and Gell classification, clinical manifestations, allergens, and characteristics. Discover the role of mediators, allergens, and treatments for immediate and delayed hypersensitivity reactions.


Hypersensitivity Reactions: Types, Manifestations, & Treatment
E N D
Presentation Transcript
Introduction • Generally the immune system is protective • Immune response resulting in exaggerated or inappropriate reaction harmful to the host • Severe damages may occur when the immune system responded in exaggerated or inappropriate form.
Classification • Coombs and Gell classification 1-Type I - immediate ( atopic, or anaphylactic) 2-Type II - antibody-dependent 3-Type III - immune complex 4-Type IV - cell-mediated or delayed
There will be typical clinical manifestations depending on the specific antigen to which the person is hypersensitive. • First contact sensitizes the individual thereby inducing antibody formation. Subsequent contacts elicit allergic response. • Types I, II, III are immediate types where as Type IV is considered as Delayed type (DH) where T-cells, Lymphokines & macrophages are involved.
Gel and Coombs classification of hypersensitivities. Type I IgE Mediated Classic Allergy Type II IgG/IgM Mediated Cytolytic Type III IgG Mediated Immune complex Disease Type IV T cell Delayed Type Hypersensitivity
Immediate Type I – Atopy, Anaphylaxis – IgE mediated Type II – Cytotoxic – IgG mediated with complement Type III – Immune complex – Arthus phenomenon, serum sickness – IgG and complement Delayed Type IV – Tuberculin type, contact dermatitis type – T cell, lymphokines, phagocytes.
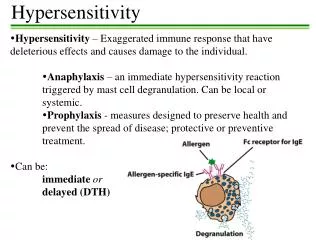
Type I - immediate (or atopic, or anaphylactic) • Type I hypersensitivity is an allergic reaction provoked by re-exposure to a specific antigen. • Immediate hypersensitivity reaction occurs when an antigen binds to IgE on the surface of mast cells or basophils. • There is subsequently release of several mediators – eg. Histamine • Initiation of the process starts when an antigen or hapten induces the formation of IgE antibody.
This antibody binds firmly with its Fc portion to basophils and mast cell surface. • Now reexposure to the same antigen results in cross linking of cell bound IgE • Degranulation and release of pharmacologically active mediators within minutes [this is immediate phase]
Exposure may be by ingestion, inhalation, injection, or direct contact • This causes an inflammatoryresponse leading to an immediate (within seconds to minutes) reaction. • The reaction may be either local or systemic. Symptoms vary from mild irritation to sudden death from anaphylactic shock.
Cyclic nucleotides and calcium play essential role in release of mediators. • Increase in cyclic GMP within these cells increases mediator release • Opposite is increase in cyclic AMP decreases the mediator release – so drugs which help in increasing cyclic AMP within these cells are used to treat type I reaction. Eg.Epinephrine which also has sympathomimetic activity.
Symptoms – edema and erythema [Wheal & flare] and itching appear rapidly because mediators like histamine are preformed. • The late phase of IgE mediated inflammation occurs approx. 6 hrs after exposure to antigen. • It is due to mediators eg. Leukotrienes [SRS-A]. • These are synthesized by the cells after degranulation. • Mediators cause influx of inflammatory cells like neutrophils and eosinophils. • Some people exhibit clinical symptoms to allergens involved in hypersensitivity reaction. Eg. Pollens, animal danders, foods [nuts, shellfish], drugs, mites, dust.
Allergens • Allergens are nonparasite antigens that can stimulate a type I hypersensitivity response. • Allergens bind to IgE and trigger degranulation of chemical mediators.
Some examples: • Allergic asthma • Allergic conjunctivitis • Allergic rhinitis ("hay fever") • Anaphylaxis • Angioedema • Urticaria (hives)
Characteristics of allergens • Small 15-40,000 MW proteins. • Specific protein components • Often enzymes. • Low dose of allergen • Mucosal exposure. • Most allergens promote a Th2 immune.
Atopy • Atopy is the term for the genetic trait to have a predisposition for localized anaphylaxis. • Atopic individuals have higher levels of IgE and eosinophils.
FceRI Triggers Release of Mediators Early mediators cause immediate symptoms e.g. histamine (preformed in granules) leukotriene C4 and prostaglandin D2 are quickly made 2' mediators
Mediators of Type I HypersensitivityImmediate effects • Histamine • Constriction of smooth muscles. Bronchiole constriction = wheezing. Constriction of intestine = cramps-diarrhea. • Vasodilation with increased fluid into tissues causing increased swelling or fluid in mucosa. • Activates enzymes for tissue breakdown. • Leukotrienes • Prostaglandins
Immediate vs Late Effects (early mediators) Early/Late Effect on lung airflow OR Wheezing
Mediators of Type I HypersensitivityPrimary MediatorsPre-formed mediators in granules • Histamine • Cytokines TNF-a, IL-1, IL-6. • Chemoattractants for Neutrophils and Eosinophils. • Enzymes • tryptase, chymase, cathepsin. • Changes in connective tissue matrix, tissue breakdown.
Secondary mediatorsMediators formed after activation • Leukotrienes • Prostaglandins • Th2 cytokines- IL-4, IL-5, IL-13, GM-CSF
Continuation of sensitization cycle • Mast cells control the immediate response. • Eosinophils and neutrophils drive late or chronic response. • More IgE production further driven by activated Mast cells, basophils,eosinophils.
Continuation of sensitization cycleEosinophils • Eosinophils play key role in late phase reaction. • Eosinophils make • enzymes, • cytokines (IL-3, IL-5, GM-CSF), • Lipid mediators (LTC4, LTD4, PAF) • Eosinophils can provide CD40L and IL-4 for B cell activation.
Localized anaphylaxisTarget organ responds to direct contact with allergen. • Digestive tract contact results in vomiting, cramping, diarrhea. • Skin sensitivity usually reddened inflamed area resulting in itching. • Airway sensitivity results in sneezing and rhinitis OR wheezing and asthma.
Systemic anaphylaxis • Systemic vasodilation and smooth muscle contraction leading to severe bronchiole constriction, edema, and shock. • Similar to systemic inflammation.
Treatment for Type I Pharmacotherapy • Drugs. • Non-steroidal anti-inflammatories • Antihistamines block histamine receptors. • Steroids • Theophylline OR epinephrine -prolongs or increases cAMP levels in mast cells which inhibits degranulation.
Treatment for Type I • Immunotherapy • Desensitization (hyposensitization) also known as allergy shots. • Repeated injections of allergen to reduce the IgE on Mast cells and produce IgG.
Treatment for Type IEffect of allergy shotsAllergen Specific Antibodies Change in amount of each isotype from more IgE to more IgG.
Type II - Cytotoxic hypersensitivity • The antibodies produced by the immune response bind to antigens on the patient's own cell surfaces. • The antigens recognized in this way may either be intrinsic ("self" antigen, innately part of the patient's cells) or extrinsic (absorbed onto the cells during exposure to some foreign antigen, possibly as part of infection with a pathogen) • The Ab IgG or IgM attach to the antigen by the Fab region and acts as a bridge to complement with its Fc portion. This results in the complement mediated lysis.
IgG and IgM antibodies bind to these antigens to form complexes that activate the classical pathway of complement activation for eliminating cells presenting foreign antigens (which are usually, but not in this case, pathogens). • As a result mediators of acute inflammation are generated at the site and membrane attack complexes cause cell lysis and death. The reaction takes hours to a day. • The reaction time is minutes to hours.
Examples • Autoimmune haemolytic anaemia • Pernicious anemia • Immune thrombocytopenia • Transfusion reactions • Hashimoto's thyroiditis • Graves' disease • Myasthenia gravis • Farmer's Lung • Hemolytic disease of the newborn
Drugs like penicillin, phenacetin, quinidine can attach to the surface proteins on RBCs and initiate Ab formation. (auto-immune antibodies - IgG ) • They can interact with RBC surface and lead to hemolysis. • The direct Coomb’s test is positive (antiglobulin test) • Drugs like quinine can attach to platelets –produce thrombocytopenia – bleeding tendency • Drugs like hydralazine may modify host tissue and induce autoantibodies directed against cell DNA resulting in disease like SLE.
Some infections e.g. Mycoplasma pneumoniae infections can induce antibodies that cross react with red cell antigens – leading to hemolytic anemias. • In Rheumatic fever –antibodies against group A streptococci cross react with cardiac tissue • Good –Pasture syndrome – Ab to basement membrane of kidneys and lungs bind to those membranes and activate complement. Severe damage to membrane also occur by the proteases generated by leukocytes attracted to the site by C5a.
Type III - immune complex • Soluble immune complexes (aggregations of antigens and IgG and IgM antibodies) form in the blood and are deposited in various tissues (typically the skin, kidney and joints) • This may trigger an immune response according to the classical pathway of complement activation. • The reaction takes hours to days to develop
Examples: • Immune complex glomerulonephritis • Rheumatoid arthritis • Serum sickness • Subacute bacterial endocarditis • Symptoms of malaria • Systemic lupus erythematosus • Arthus reaction
Usually these immune complexes are scavenged by the reticulo- endothelial systems, but occasionally they persist and are deposited in the tissues leading to many disorders. • In persistent viral or bacterial infections, immune complexes maybe deposited in organs like kidneys and result in damage. • In auto-immune disorders “self” antigens may elicit antibodies that bind to organ antigens or deposit in organs as complexes e.g. joints causing arthriti, kidneys causing nephritis or blood vessesls causing vasculitis.
Wherever these complexes are deposited they trigger the complement system. • PMNLs are attracted to the site and hence inflammation and tissue injury occur • Examples of typical type III reactions include- 1. Arthus reaction 2. Serum sickness
1. Arthus reaction • Arthus described. • The inflammation by deposition of immune complexes at a localized site or. • First the animal is injected with antigen repeatedly till they have a high level of IgGAb • Second the same antigen is injected subcutaneously or intradermally • Intense edema hemorrhage develop reaching peak 3-6 hrs i.e. localized inflammation • Much more Ab is required for Arthus reaction
2. Serum sickness • Arthus reaction is localized inflammation whereas serum sickness is a systemic inflammatory response to the presence of immune complexes deposited in many areas of the body. • After the injections of foreign serum (nowadays commonly drugs) the antigen is excreted slowly. • During this time Ab production starts. So there is simultaneous presence of Ag as well as Abs that leads to immune complex formation which are circulated and deposited into various sites.
Typical reaction presents with fever, urticaria, arthralgia, lymphadenopathy, splenomegaly, eosinophilia occurring a few days to 2 weeks after injection of foreign serum or drug. • Several days are required for the symptoms to appear but still classified as immediate because symptoms occur as soon as the immune complexes are formed. • Symptoms improve as soon as the immune system removes the antigen or subsides when antigen is eliminated.
Type IV Hypersensitivity • Type IV hypersensitivity is often called delayed type as the reaction takes two to three days to develop. • Unlike the other types, it is not antibody mediated but rather is a type of cell-mediated response. • This can be transferred by immunologically committed T cell (sensitized) and not by serum. • Tuberculin type and contact dermatitis type
Some clinical examples: • Contact dermatitis(eg, poison ivy rash) • Temporal arteritis • Symptoms of leprosy • Symptoms of tuberculosis • Transplant rejection
Clinically important Delayed Hypersensitivity reactions A. contact hypersensitivity- • Cell mediated hypersensitivity occurs after contact with simple chemicals like nickel, formaldehyde, plant materials – poison ivy, poison oak, topically applied drugs like sulfonamides, neomycin, sometimes cosmetics, soaps and others. • In all these cases small molecules act as hapten, enter the skin, attach to the body proteins to become complete antigen.
It is presumed that the normal skin proteins to which the immune system is tolerant act as a carrier protein. The hapten now alters the protein and the immune system starts recognizing it as foreign. • Cell mediated hypersensitivity is induced particularly in the skin, so sensitization • Later skin contact with the offending agent leads to the development of eczema, erythema, itching, vesicles or necrosis of skin within 12-48 hours. • Sometimes the antigen can be identified by patch testing. Subsequently the offending agent can be avoided to prevent recurrences
Tuberculin type- • Antigen of microorganism can cause Delayed Hypersensitivity. So it can be made use of in the diagnosis. E.g. Tuberculin test. • A patient previously exposed to M.tuberculosis is injected with a small amount of Tuberculin (PPD) intra-dermally. There will be no reaction in the first few hours. Gradually induration and redness develop and it peaks 48-72 hours. This means a positive test.
A positive skin test indicates the person has been infected with the agent but it does not confirm the presence of current disease. But if skin test converts from negative and positive, it suggests that the patient has been recently infected. • Infected persons need not always have a positive skin test. E.g. overwhelming infections, disorders which suppresses Cell Mediated Immunity , AIDS or administration of immune-suppressive drugs like corticosteroids, anti-neoplastic agents can cause anergy.
A positive skin test response assists in diagnosis – supports chemoprophylaxis or chemotherapy • Examples- 1. Leprosy – Lepromin test • Positive test indicates Tuberculoid type with competent CMI. • Negative test indicates Lepromatous leprosy with impaired CMI.