Mechanism
Polycystic Kidney Disease Group 32: Priya Tanna , Mona Dave, Niccole Kleeman, Pejman Solaimani, Rushi Parikh. Mechanism.

Mechanism
E N D
Presentation Transcript
Polycystic Kidney DiseaseGroup 32:Priya Tanna , Mona Dave, Niccole Kleeman, Pejman Solaimani, Rushi Parikh
Mechanism • Polycystic kidney disease (PKD) is a genetic disorder where numerous cysts, or fluid-filled sacs, form on the kidneys. Due to these cysts, the kidneys become fairly enlarged, damaging the normal kidney tissue and eventually leading to kidney failure. PKD is an inherited disease that can present in two forms, autosomal dominant and autosomal recessive. Autosomal dominant PKD is the most common form of the disease and it can be associated with two separate genes. Most patients inherit a defective copy of the PKD1 gene on chromosome 16, while the remaining patients inherit a defective copy of the PKD2 gene on chromosome 4. Mutations in these genes can either be caused by frameshift, deletion, or missense mutations. Autosomal recessive PKD is a more rare form of the disease that affects mostly infants and young children.
Presentation of the Disease • There are various symptoms that a patient with Polycystic Kidney Disease displays. The most common include back pain, side pain, and headaches. In addition to these symptoms, one can also experience high blood pressure, frequent kidney and urinary tract infections, kidney stones, abnormal heart valves, aneurysms in the brain, diverticulosis, and hematuria (blood in the urine). In most cases, PKD is of a mild form, where patients can lead a normal life, however in severe cases, PKD can lead to kidney failure where dialysis and kidney transplants are necessary treatments. There is no cure for Polycystic Kidney Disease, however there are treatment options that are available to ease symptoms. Over-the-counter medications can be used to decrease pain and antibiotics can help treat kidney and urinary tract infections. Finally, medications are available to lower blood pressure, however proper diet and exercise are the best options in blood pressure control.
Pathology Slides Adult Polycystic Disease (Note the lack of Glomeruli) Image from University of Iowa Pathology Slide Box Polycystic Disease Image from University of Iowa Pathology Slide Box
Higher Magnification - Adult Polycystic Disease Image from Universityof Iowa Pathology Slide Box Cyst with low cuboidal/low columnar epithelium
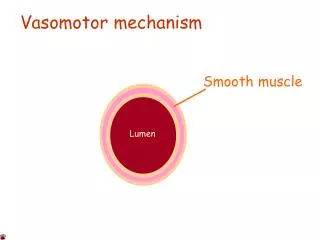
Function of Macula Densa in Urine Production • Macula densa cells are specialized cells located at the end of cortical thick ascending limb and the beginning of the distal tubule of the nephron. This segment of the renal tubule is impermeable to water and has Na:K:2Cl co-transporter which in turn is responsible in diluting the tubular fluid and maintenance of the salt and water balance. In addition, Macula densa cells play an important role in regulating the blood pressure by controlling the release of renin from granular cells, a process that is called tubulo-glomerular feedback (TGF). Initiation of TGF is dependent of the change in the composition of the luminal fluid which is detected by Macula Densa cells. • Macula densa cells can detect and vary the levels of luminal sodium chloride concentration and osmolarity as the filtrate is delivered from the previous portions of the nephron. The primary means for NaCl to enter into the macula densa is the Na/K/2Cl cotransporter which is located at the apical membrane. Also, it has been shown that there are three splice variant of this cotransporter: A, B, F. Indeed, macula densa cells express the B variant which has high affinity and low capacity for sodium chloride. This allows the macula densa to further re-absorb NaCl which has not been re-absorbed in previous segment and is in the low concentration.
Macula Densa continued • Macula densa cells also play an important role in regulating the blood pressure. Indeed, when the blood pressure decreases, there will be less glomerular filtration which in turn leads to a decrease in the concentration of sodium chloride in the lumen of nephron. This reduced concentration of sodium chloride is detected by the osmoreceptors located in the macula densa cells of distal tubules and results in release of renin from the granular juxtaglomerullar cells located at the afferent arterioles. It is also believed that biosynthesis of prostaglandin is the mediator of renin release by macula densa cells. On the other hand, it has been shown that in case of increased sodium chloride concentration in the luminal fluid, macula densa cells may produce adenosine which in turn inhibits release of renin from the juxtaglomerullar granular cells. Renin hydrolyses angiotensinogen (a blood-borne glycoprotein that is made and secreted by liver) and converts it to angiotensin I. Subsequently, angiotensin I circulates in blood and is cleaved and converted to octapeptide angiotensin II by converting enzymes in the lung. Subsequently, Angiotensin II acts on multiple target in order to restore the blood pressure. Firstly, it stimulates the zona glomerulosa cells of the adrenal cortex to secrete Aldostrone. Aldostrone in turn increase the sodium re-absorption from the distal tubule and the cortical collecting tubule. This also results in passive re-absorption of water which leads to the more concentrated (less volume) urine. Secondly, Angiotensin II directly affects the distal tubule to increase the reuptake of sodium and water which further concentrate the urine. Thirdly, Angiotensin II results in constriction of afferent and efferent renal constriction which leads to increase in blood pressure. Therefore, macula densa cells results in a more concentrated urine production to compensate for a drop in the blood pressure by interacting with juxtaglomerullar complex and regulating the release of renin from granular cells.