Optimal Nutrition for Performance and Health
Understand the vital role of nutrition in exercise, injury prevention, weight control, and overall well-being. Essential vs. Nonessential Nutrients, Dietary Recommendations, and Recommended Allowances discussed.

Optimal Nutrition for Performance and Health
E N D
Presentation Transcript
chapter1 Introduction to Nutrition for Exercise and Health chapter 1 Introduction to Nutrition for Exercise and Health Prof Jennifer Broxterman, RD, MSc FN3373: Nutrition for Physical Activity Lecture 1 Author name here for Edited books
Sports Nutrition Introduction • Proper nutrition can help: • Improve exercise performance • Decrease recovery time from strenuous exercise • Prevent exercise-associated injuries due to fatigue • Provide the fuel required during times of high-intensity training • Control weight • Help reduce the risk of numerous chronic diseases • T2DM, CVD, hypertension, obesity, osteoporosis, some cancers
Role of Nutrition in Exercise & Sport • Nutrition plays a vital role in exercise performance and training • Benefits both competitive and recreational athletes • Good nutrition is especially important for athletes who: • Compete in sports tournaments • Engage in strenuous PA on a daily or more than daily basis • Examples?
Injury Reduction • Risk of injury during exercise • Fuel & hydration status impacts level of fatigue and ability to concentrate • Risk of injury post-exercise • Proper nutrition can help speed the healing process for injured athletes • Surgery / Bone Injuries: requires extra kcal & nutrients, including protein, vitamins, and minerals
Weight Control / Body Composition • Nutrition plays an important role in weight control and body composition • Few individuals are happy with their weight, body fat levels, or body shape • Realistic expectations can improve health and quality of life and reduce stress levels • Disordered eating tendencies tend to be higher in athletes than the general population, esp. women
Essential vs. Nonessential Nutrients • Discovery • Evolved from observations that certain diseases occurred in populations that consumed poor diets • Able to show that including specific foods in the diet could correct or prevent the diseases • Essential nutrients: food constituents that prevent disease or health problems (“indispensible”) • Nonessential nutrients: nutrients that could be deleted from the diet with no adverse health effects (“dispensable”) • E.g. physiologically essential nutrient for the body but classified as a nonessential nutrient?
Conditionally Essential Nutrients • Conditionally essential: some “essential” nutrients are synthesized by the body from precursors, and interactions between nutrients could alter requirements • Potentially affected by: • Some disease states • Genetic defects • Stress • Illness • Aging
Conditionally Essential Nutrients • Criteria to establish the conditional essentiality of a nutrient: • The plasma concentration of the nutrient declines into the subnormal range, although the body should be able to synthesize the nutrient. • Chemical, structural, or functional abnormalities appear that are associated with low blood concentrations of the nutrient. • Dietary supplementation of the nutrient returns plasma concentrations to normal and corrects the abnormalities seen when blood concentrations are low.
Desirable & Beneficial Nutrients • Nonessential nutrients that are important for good health and disease prevention • New nutrient category: “desirable or beneficial for health” (Carpenter and Harper, 2006) • Examples: fibre, phytochemicals, carotenoids, amino acid derivatives • Are NOT classified as essential or conditionally essential nutrients
Dietary Reference Intake (DRIs) DRIs EAR RDA AI UL
Nutrition Recommendations • Yardsticks used as standards for measuring healthy people’s energy and nutrient intakes • Used to: • Assess nutrient intakes • Make recommendations on amounts to consume • Standards in the Canada and U.S. are the Dietary Reference Intakes (DRI) • Estimated Average Requirements (EAR) • Recommended Dietary Allowances (RDA) • Adequate Intakes (AI) • Tolerable Upper Intake Levels (UL)
Goals of the DRI Committee • Setting Recommended Intake Values (RDA, AI) • Facilitating Nutrition Research and Policy (EAR) • Establishing Safety Guidelines (UL) • Preventing Chronic Disease
Goal 1: Setting Recommended Intake Values • RDA: based on solid experimental evidence and reliable observation • nutrient intake goals for individuals • derived from EAR • meets requirement of 97-98% of individuals in a life stage and gender group • AI: also as scientifically based as possible, but setting them requires some educated guesses • established whenever scientific evidence is insufficient to generate an RDA
Goal 2: Facilitating Nutrition Research & Policy • EAR: nutrient requirements for given life stages and gender groups that researchers and nutrition policymakers use in their work • Public health officials may also use them to assess nutrient intakes of populations and make recommendations • EAR values form the scientific basis upon which the RDA values are set
Goal 3:Establishing Safety Guidelines • UL • Identify potentially hazardous levels of nutrient intake • Useful to consumers who take supplements or consume foods or beverages to which vitamins or minerals have been added • Public health officials rely on UL values to set safe upper limits for nutrients added to our food and water supply
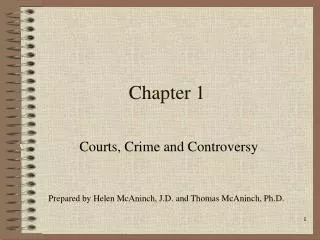
The Naive View vs. Accurate View of Optimal Nutrient Intakes
Goal 3:Establishing Safety Guidelines • People’s tolerances for high doses vary • Caution is in order when nutrient intakes approach UL values • Some nutrients do not have UL values • Does not imply that it is safe to consume it in any amount • Only means that insufficient data exists to establish a value
Goal 4:Preventing Chronic Disease • The DRI committee takes into account chronic disease prevention, wherever appropriate • healthy ranges of intake for carbohydrate, fat, and protein • Acceptable Macronutrient Distribution Ranges (AMDR) • 45%-65% from carbohydrate • 20%-35% from fat • 10%-35% from protein
Understanding the DRIs • Government funded • Based on recent scientific research whenever possible • Optimal intakes NOT minimal requirements • Generous margin of safety • Meet needs of virtually all healthy people within a specific gender and age group • Based on specific indicators of nutrient adequacy • Normal growth and development • Optimal blood nutrient concentrations • Reduction of certain chronic diseases and disorders
Understanding the DRIs • Daily intakes to be achieved on average, over time • Assume intakes will vary from day-to-day • Set high enough to ensure that nutrient body stores will meet nutrient needs (from 1 day to 3 months based on the nutrient) • Apply to healthy persons only • Health maintenance and disease prevention • Not restoration of health • Separate recommendations gender, age, lifecycle • Differences between men, women, pregnant and breastfeeding women, children and other life stage groups
Setting Energy Requirements • Estimated Energy Requirements (EER) • The average dietary energy intake predicted to maintain energy balance in a healthy adult of a certain age, gender, weight, and level of physical activity with consistent good health • Value is not generous • Is set at the average of the population’s estimated energy requirements • Enough food energy is critical to support health and life • Too much energy causes unhealthy weight gain • The DRI committee did not set a UL for energy
Eating Well with CFG (2007) • To help people achieve goals set forth by Canada’s Guidelines to Healthy Eating, Health Canada provides a food group plan • Diet planning tool • Sorts foods into groups based on their nutrient content • Specifies that people should eat a minimum # of servings of foods from each group
Variations of Food Guides • Many countries have their own nutrition organizations that develop dietary guidelines, reference intakes, and food guide pyramids, rainbows, circles, etc. • Goal is to meet the dietary needs of the particular population • Must consider: • cultural aspects related to food • eating patterns • lifestyle factors
Mediterranean Diet for Athletes • Endurance athletes • Marathon & ultra-endurance athletes • Higher fat diet (~40%) • Replacement of intra-muscular fat used as a fuel source during exercise • Best food sources: nuts, seeds, olive oil, fish • Athletes with lower energy requirements • Offers a nutrient-dense diet • Reduce total fat from olive oil, cheese, & nuts but maintain high intake of V&F, whole grains, lean protein
Food Pyramid for Athletes • Swiss Forum for Sport Nutrition • Builds on the Basic Food Pyramid used in Switzerland, designed for the normally active • Covers the extra energy and nutrient requirements incurred by the demands of daily exercise training • Carefully considered the volume and intensity of various sports • Feasibility of consuming the extra servings for each food group was also considered for athletes in “real-life” settings • Sport-specific foods, fluids, and recovery products were also integrated
Figure 1.6 (continued) Sweets Oils/Fats Protein Grains V&F Fluids
Canadian Physical Activity Guidelines (NEW in 2011) • Canadian Society for Exercise Physiology www.csep.ca/guidelines Children (5-11 y) Youth (12-17 y) Adults (18-64 y) Older Adults (65 y and older) • New guidelines should be viewed as a minimal target • Evidence-based, realistic and achievable • To promote healthy active living for the Canadian population • Levels of PA & fitness have dropped dramatically • Overweight/obesity in Canadian has been steadily increasing • Steady rise in diseases associated with overweight & obesity
Children (5-11 y) & Youth (12-17 y) GUIDELINES • For health benefits, children aged 5-11 and youth aged 12-17 years should accumulate at least 60 minutes of moderate-to-vigorous-intensity PA daily. This should include: • Vigorous-intensity activities at least 3 days per week • Activities that strengthen muscle and bone at least 3 day per week • More daily PA provides greater health benefits
Adults (18-64 y) GUIDELINES • To achieve health benefits, adults aged 18-64 years should accumulate at least 150 minutes of moderate-to-vigorous-intensity aerobic PA per week, in bouts of 10 minutes or more • Beneficial to add muscle and bone strengthening activities using major muscle groups, at least 2 days/week • More PA provides greater health benefits
Older Adults (65+ y) GUIDELINES • To achieve health benefits and improve functional abilities, adults aged 65 years and older should accumulate at least 150 minutes of moderate-to-vigorous-intensity aerobic PA per week, in bouts of 10 minutes or more • Muscle and bone strengthening activities using major muscle groups at least 2 days/week • Those with poor mobility should perform PA to enhance balance and prevent falls • More PA provides greater health benefits.
Rationale for New PA Guidelines • Explosion of new research in recent years • Old guidelines were out-of-date • Evidence to support more specific recommendations • Some age ranges missing with old guidelines • More robust guideline development processes now • Inactivity crisis deserves up-to-date guidelines
Canadian Sedentary Behaviour Guidelines for Children & Youth The scientific evidence showed that: • Being sedentary for more than 2 hours per day was associated with: • Unfavourable body composition • Decreased fitness • Lowered scores for self esteem and pro-social behaviour • Decreased academic achievement
Canadian Sedentary Behaviour Guidelines for Children & Youth GUIDELINES For health benefits, children (aged 5-11 y) & youth (aged 12-17 y) should minimize the time they spend being sedentary each day. This may be achieved by: • Limiting recreational screen time to no more than 2 hours per day; lower levels are associated with additional health benefits • Limiting sedentary (motorized) transport, extended sitting and time spent indoors throughout the day