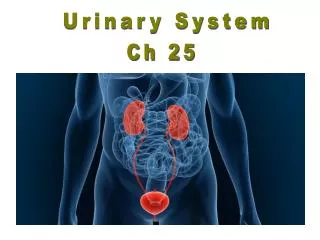
Urinary System
Urinary System. Chapter 24 – Day 2. Review Nephron Structure. Network with blood vessels Two types of nephrons Cortical Nephrons – loop of Henle does not extend below cortex Juxtamedullary nephrons – loop of Henle extends into medulla Vasa recta – feature of jextamedullary nephrons

Urinary System
E N D
Presentation Transcript
Urinary System Chapter 24 – Day 2
Review Nephron Structure • Network with blood vessels • Two types of nephrons • Cortical Nephrons – loop of Henle does not extend below cortex • Juxtamedullary nephrons – loop of Henle extends into medulla • Vasa recta – feature of jextamedullary nephrons • 85% are cortical nephrons • Majority of process is done here • 15% are juxtamedullary • Important role in concentrating urine • Conserving water in the body
Renal corpuscle • Renal arteries branch into afferent arterioles in the cortex • One afferent arteriole enters the renal corpuscle • Wall of the renal corpuscle is the Bowman’s capsule • Afferent arteriole branches into capillary network • Glomerulus, inside the corpuscle within the bowman’s capsule • A second efferent arteriole connects to the glomerulus – brings blood out of the renal corpuscle • (Efferent arteriole is thinner than afferent) • Efferent arteriole branches around nephron as peritubular capillaries and vasa recta • Eventually the efferent arteriole connects to venules – carries blood to renal veins and out of the kidney
Nephrons & blood supply Fig. 24.7
Kidneys – Blood supply Fig. 24.5
Glomerulus • Surrounded by 2 layers • Bowman’s capsule: • Visceral epithelium • Parietal epithelium • Separated by capsular space • Blood in the glomerulus is bounded by 2 walls • Endothelial cells of the blood vessels • Visceral layer of the bowman’s capsule Fig. 24.8
Glomerulus • Endothelial cells of blood vessels • Have large diameter pores: • Fenestrations • Basement membrane • Visceral Layer of the Bowman’s capsule • Special basement membrane = lamina densa • Special cells = podocytes • These have special feet like structures called pedicels • Spaces between pedicels = filtration slit/slit pore • Special structures of the endothelial cells and visceral layer restrict the passage of particles according to size (analogous to the filter paper) • Capsular space = place where filtrate is released
Glomerulus - barriers Fig. 24.8
Glomerulus blood boundaries Fig. 24.8c
Filtration in the Glomerulus • Blood rushes into glomerulus via the afferent arteriole • Difference in diameter between afferent & efferent arterioles results in High Blood Pressure inside the Glomerulus • = Effective Filtration Pressure (EFP) • This pushes blood against the endothelial cells • Filtration takes place • Fenestrated capillaries – stops blood cells from passing through, but all other contents go through • Basement membrane – stops large proteins • Pedicels/filtration slits – stops medium-sized proteins from leaving blood
Glomerular Filtration Fig. 24.10
Filtrate • Remaining contents end up in the capsular space and are called filtrate • Contents of filtrate: • Water • Small proteins • Glucose • Amino acids • Vitamins • Citric acid • Ions: Na+, Cl-, K+, HCO3 • ammonia • Urea • Bilirubin • Neurotransmitter • Hormones
Filtrate - PCT • Filtrate passes to proximal convoluted tubule (PCT) • PCT walls = simple cuboidal epithelium • Outside fluid = peritubular fluid • Then peritubular capillaries • PCT – reabsorption begins • 99% of the reabsorption is of organic materials • Glucose, amino acids, vitamins, citric acid • Facilitated diffusion • Transport of Ions = active transport & passive • Water reabsorption = osmosis • Enters peritubular fluid, then to capillaries
Filtrate – Loop of Henle • Tubular fluid with remaining contents flows into Loop of Henle • Descending & Ascending Limbs • Juxtamedullary nephrons – in contact with the vasa recta • Reabsorption of water & solutes • (specifically Na+ & Cl-) • Descending & Ascending limbs have different properties – very important in concentrating urine
Loop of Henle • Descending limb = thin • Permeable to H2O • Mostly impermeable to salts (Na+,Cl-) • Ascending limb = thick • Impermeable to H2O and solutes • Prevents diffusion by concentration gradient • Allows selective permeability • Only Na+& Cl- can leave via active transport while wastes stay in • Salts (Na+,Cl-) are pumped out by active transport = reabsorption of Na+& Cl- into blood Fig. 24.13
Loop of Henle • As tubular fluid moves up, salts enter peritubular fluid via active transport into vasa recta • Results in a high solute concentration of peritubular fluid • Know: • Direction of H2O? Direction of salts? • From which limb? • What is the significance/importance? • How does the countercurrent work? Fig. 24.13
Loop of Henle • Countercurrent flow drives reabsorption • Osmotic concentration is constantly maintained • Allows reabsorption of H2O into blood b/c osmotic concentration is high in the peritubular fluid (due to high salts) • = contercurrent multiplication (exchange increases) • Loss of H2O from descending limb concentrates solutes in urine • Tubular fluid containing mostly wastes & some ions enters distal convoluted tubule (DCT)
Filtrate – Distal Convoluted Tubule • Further reabsorption of salts (Na+ & Cl-) • Active and Passive • Presence of aldosterone alters rate of Na+ reabsorption • Ca2+ may be reabsorbed depending on calcitriol • Secretion also occurs in DCT • Wastes are not reabsorbed – moves forward to collecting tube Fig. 24.15
Filtrate – Distal Convoluted Tubule • Further reabsorption of salts (Na+ & Cl-) • Active and Passive • Presence of aldosterone alters rate of Na+ reabsorption • Ca2+ may be reabsorbed depending on calcitriol • Secretion also occurs in DCT • Wastes are not reabsorbed – moves forward to collecting tube Fig. 24.15
Urinary System Chapter 24 – Day 3
Nephron - Secretion • Reabsorption & secretion take place in the DCT • Secretion: • Other wastes that did not enter the nephron during filtration • Transported later by secretion • Peritubular capillaries → nephron • PCT & DCT are involved in secretion • K+ and H+ ions – depends on blood levels/blood conditions • Example: H+ ions increase from CO2 conversion, they are secreted to maintain balance • Diabetes: ketones are released = acidic, so more H+ is secreted • NH4+ ions (comes from removal of NH3 group from amino acids) • Other secreted compounds = drugs, creatinine, neurotransmitters
Filtrate – Collecting Duct • Urine moves into the collecting tubule (urine) • Some reabsorption: • Na+ ions • HCO3- ions • Some urea reabsorption (helps to maintain high salt concentration in peritubular fluid) • Concentration gradient is very important to keep the flow of things moving properly • Ions & H2O enter peritubular fluid, then go to vasa recta • Keeps a constant concentration gradient of high salt levels in the peritubular fluid • H2O reabsorption in kidney = very important process • Helps to keep H2O balanced in the body • Depends on solute concentration
Urine - hydration • If the body is well hydrated H2O absorption occurs only in the descending limb of Loop of Henle • Solute concentration gradient in Loop of Henle & Collecting Tubule** Fig. 24.13
Urine - hydration • Dilute urine = large volume because high amounts of water are retained • Only ions are reabsorbed heavily • If the body is dehydrated – activates pituitary gland to produce antidiuretic hormone (ADH) • Body conserves H2O in the kidney & thirst response for more H2O intake • Special H2O channels open in collecting tubule • H2O is reabsorbed from collecting tubule • Driven by diffusion because salt concentration is already high outside • Yields concentrated urine – small volume (conc. urea) • Diuretics like caffeine: • Prevent H2O reabsorption in collecting tubule, force H2O out of cells • Leads to dilute urine but reduces blood volume • Are also used to alter blood pressure
REVIEW & LEARN Fig. 24.16
REVIEW & GET THE “GIST” Fig. 24.17
Urine Collection and Reabsorption • After filtration, reabsorption & secretion – urine is produced • From the papillary duct it enters the minor calyx • There it joins with other to form the major calyx • Then it joins the renal pelvis Fig. 24.7, 24.4
Urine Collection and Reabsorption • Urine collects in the renal pelvis • Urine is then delivered & eliminated through the urinary tract: • Ureters • Transport • Urinary bladder • Storage • Urethra • Elimination Fig. 24.1
Ureters • Ureters are 30cm long, muscular tubes • Ureters are attached to the posterior wall of the abdomen • Ureters are arranged differently in men & women because the placement of the bladder is different in men and women Fig. 24.19
Urinary Bladder • The urinary bladder is a highly muscular organ • Inside layer = transitional epithelium • This permits stretching of the bladder without damage to the surface cells • The urinary bladder is held in place with the help of ligaments • The region near the neck • = Inner urethral sphincter • Under involuntary control • The neck leads to the urethra Fig. 24.19c
Urethra • The urethra is placed in different places in males and females • Males – from bladder to penis • Females – short urethra, located at the front of the vagina Fig. 24.19
Urethra • At the end of the urethra is the external urethral sphincter • This is a muscular sphincter ~ valve • Voluntary control • As pressure builds up against pressure – sensitive receptors in bladder • The external sphincter relaxes – this opens the internal sphincter & urine is eliminated Fig. 24.19c
Urethra • At the end of the urethra is the external urethral sphincter • This is a muscular sphincter ~ valve • Voluntary control • As pressure builds up against pressure – sensitive receptors in bladder • The external sphincter relaxes – this opens the internal sphincter & urine is eliminated Fig. 24.19c
Urine Elimination – Neural Control Fig. 24.21
Kidney Problems Glomerular Nephritis • Caused by inflammation of the glomerulus • How does that inflammation occur? • Allergic reaction, bacterial infection, other pathogens lead to an inflamed, swollen glomerulus • Filtration is affected • There is less of a “block” to the permeability of endothelial cells and capsular membrane • More RBCs and proteins end up in the filtrate • Degree of affliction: acute to minimal
Acute Glomerular Nephritis • Typical cause: • Strep. infection elsewhere in the body • Glomerulus produced inflammatory response due to antibody/antigen complex • Most common in children and young adults • Symptoms • Fever, chills, nausea, edema, urinary failure • Can result in kidney failure • Treatment: • Drugs to eliminate antibody/antigen complex • Steroids to reduce inflamation • Rest • Glomerular lesions already present will not heal
Urinary Tract Infection • Very common, especially in females • Cystitis = infection in urinary bladder • Urethritis = infection in urethra • Pyelonephritis = infection in the kidney • Symptoms: • Back pain, fever, nausea, discharge • Urgency to urinate • Frequent urination • Causes: • Bacterial infection (entered at urethra) • Treatment • Antibiotics
Incontinence • Lack of bladder control • Urinary sphincters cannot control passage of urine • May be psychological or physiological • Incontinence • Causes: • muscle damage to sphincter • Nerve damage (surgery or tumor) • Medications &/or stress • Treatments (adult patients) • Kegel exercises to improve sphincter muscle tone • Electrical stimulations to suppress bladder contractions • May just need absorptive pads • Read about urine retention p749 for developmental stages - Enuresis (bed wetting)
Kidney Problems – Kidney Stones • Kidney stones = renal caliculi • Salt exchange happens in the kidney, thus crystals can be formed • Normally, protein acts as a crystal growth inhibitor • If abnormal conditions exist: • Crystal growth is not prevented – growth in renal pelvis • Mostly kidney stones are precipitated Ca2+ salts like CaPO4 • These can get trapped in the ureter and this causes severe pain
Kidney Problems – Kidney Stones • Causes of Kidney Stones: • No inhibition • Dehydration • Excess Ca2+ intake • “Hard” water • Oaxalates • Treatment • Observe kidney stones on pyelogram (use dye for urinary tract) • Pass the stone? • Vibration to break apart crystals • Extracorporeal shock wave lithotripsy http://www.webmd.com/kidney-stones/extracorporeal-shock-wave-lithotripsy-eswl-for-kidney-stones
Renal Failure • Acute & Chronic • Hemodialysis • Read about it 745-746
Kidneys – Blood supply Fig. 24.7
Kidneys – Blood supply Fig. 24.8
Kidneys – Blood supply Fig. 24.5
Kidneys – Blood supply Fig. 24.5