Download
1 / 18
180 likes | 265 Vues
This case study involves a 21-year-old female with a history of a slowly enlarging, firm, occasionally tender scalp mass. Admitted for evaluation, the patient has a family history of hypertension and diabetes. On physical examination, no alarming symptoms were noted, but a soft tissue tumor possibly due to recurrent hemangioma or rare Merkel cell carcinoma is considered. This text discusses the characteristics, diagnosis, and prognosis of Merkel cell carcinoma, emphasizing the importance of early detection and appropriate management.

E N D
J.M. 21 y/o female cc: scalp mass
History of Present Illness • Slowly enlarging, firm, occasionaly tender mass on R parietoocipital area (3x3cm) • Consult • A: Hemangioma • P: Excision 14years PTA
2 mos PTA • Recurrence of slowly enlarging mass (5x5cm) • Consult at UST OPD • Scalp X Ray • Ultrasound of neck ADMISSION
PAST MEDICAL HISTORY • (-) HPN • (-) DM • (-) HPV infection • (-) Asthma • (-) Allergies • (-) PTB
PERSONAL AND SOCIAL HISTORY • Mixed diet • Nonsmoker • Not an alcoholic beverage drinker
FAMILY HISTORY • (+) HPN – mother • (+) DM – grandfather • (-) Asthma • (-) CA
REVIEW OF SYSTEMS • (-) weight loss, weakness, fatigue • (-) Headache, dizziness, blurring of vision • (-) hearing loss, aural discharge, tinnitus • (-) epistaxis, nasal discharge, sinusitis • (-) hoarseness, mouth sores, dysphagia • (-) dyspnea, cough
PHYSICAL EXAMINATION • Conscious, coherent, ambulatory, not in distress • BP: 120/80 PR 80bpm RR 18cpm T 36.5°C Wt. 60 kg Ht. 162cm • Warm moist skin, no active dermatoses • Pink palpebral conjunctivae, anicteric sclerae • No naso-aural discharge, non-congested turbinates, non-tender sinus, buccal mucosa, tonsils not enlarged, no bleeding gums • Supple neck, (-) palpable cervical Lymph Nodes, no thyromegaly
Symmetric on chest expansion, (-) retractions, lungs resonant, clear breath sounds • Adynamic precordium, AB 5th LICS MCL, S1>S2 at the apex, S2>S1 at the base, no murmurs • Flat abdomen, no organomegaly, (-) rebound tenderness, no masses • (-) pallor, clubbing, petechiae, ecchymoses • Pulses ++ on all extremities
Admitting Impression • Soft tissue tumor to consider recurrent hemangioma vs. granuloma
Merkel’s Cell Carcinoma • Classified as a neuroendocrine malignancy of the skin. • Cutaneoussmall cell undifferentiated carcinoma • Incidence of 1200 per year in the US • Mortality rate of 33 % • National Cancer Institute. Fact Sheet MERKEL’S CARCINOMA. 2007 • Merkel Cell Carcinoma: More Deathsbut Still No Pathway to Blame Bianca Lemos and Paul Nghiem. Journal of Investigative Dermatology (2007)
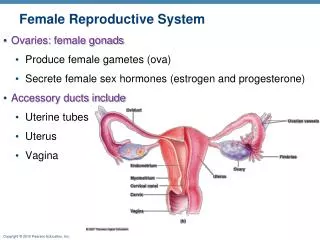
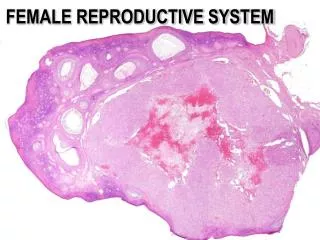
Discussion • Merkel’s cells located in the basal layer of the epidermis. • Grossly, the primary tumor presents as a small, red, pink, or blue-violet, non-ulcerated, painless, intradermal nodular mass often located in sun-exposed areas of the skin such as the head and neck
Discussion • Neuroendocrine markers • Neuron-specific enolase • Chromogranin • Synaptopysin Merkel cell carcinoma, VirveKoljonen. World Journal of Surgical Oncology 2006
American Joint Committee on Cancer • Stage I (primary lesion ≤ 2 cm) • Stage II (primary lesion > 2 cm). • Stage III (nodal involvement) • Stage IV disease(metastatic)
Prognosis • Aggressive course with reported overall 5-year survival rates ranging from 30% to 64%. • Survival after a diagnosis of MCC is highly dependent on the stage at presentation. • 90 percent of recurrences occurring within three years of diagnosis • Merkel Cell Carcinoma: A Case Report and Literature Review. Oncology. Medical Journal of Islamic World Academy of Sciences 15:3, 91-94, 2005