Download
1 / 36
810 likes | 3.29k Vues
A Brief History of Cataract Surgery. Normal Eye Anatomy. The lens is the focusing mechanism of our eye – as we age it gradually clouds, making our vision fuzzy.

E N D
Normal Eye Anatomy • The lens is the focusing mechanism of our eye – as we age it gradually clouds, making our vision fuzzy. • The lens is held in place by zonules – fragile microscopic cables that we try to preserve during surgery and use to support the new lens
Terms • Couching – a sharp instrument is plunged into the eye, pointed into the whitish opacity, and pushed down to dislodge the cataract • Intracapsular Cataract Extraction – the zonules are broken and the entire lens is removed • Extracapsular Cataract Extraction – the nucleus and cortex are removed, preserving the zonules and posterior capsule
Cataract Surgery The development of cataract surgery proceeded in spurts – we can trace the insights of a few brilliant, creative people that have given us the modern cataract surgery technique we enjoy today
Four eras of cataract surgery • Couching – 600 BC to the mid 17th century • Daviel /ECCE– 18th century • ICCE – 19th century to 1970’s • ECCE – 1960 to present
Instruments • Until the invention of the slit-lamp by Gullstrand in 1910 and the ophthalmoscope by Von Helmholtz in 1951, the eye examination was limited to the external eye and pupil.
Cataract • First described as early as 600 BC • Early physicians thought of cataracts as a coagulation of the eye humors behind the iris • ConstantinusAfricanus (AD 1018) a monk and Arabic oculist introduced the term cataract by translating the Arabic equivalent of “suffusion” into the Latin “cataracta” which meant “waterfall”
Couching • Early cataract surgery started in India and Greece – 600 BC • Couching surgical instruments found in Egyptian tombs – suggests “surgeons” specialized in couching • Egypt – 250 BC – first well described surgery with pictures of instruments • Couching initially performed by dedicated specialists with no formal medical training • Couching is still practiced in some part of the world including Africa
Couching is one of the most effective surgeries of ancient times. The name comes from couching: lowering a spear or lance to a horizontal position in preparation for an attack • Approximately 20% of patients gained some sight
Written accounts of cataract surgery Indian physician Sushruta wrote SushrutaSamhita (6 century BC)– ancient Sanskrit manual for surgery – book 6 describes cataract surgery. Information travelled west to Greece and east to China Celsus – Latin Encyclopedist at time of Christ – wrote De Medicinae - describes cataract surgery
Dark Ages (5th-15th Century) • A time of chaos and wars – the knowledge of couching lost in Europe
Midevil Europe • 1443 Pope Nicholas discovered the text of Celsus – the knowledge of couching re-emerged • Eye surgeons were lower class Oculists – relied on showmanship – part of travelling fairs – initially surgeries were successful, followed in weeks by progressive inflammation and loss of vision. By then the oculists had moved on.
Renassance (14-17th Centuries) • Doctors learned surgery and became specialists – couching still only form of cataract surgery • 1650’s – Rolfink in Germany dissected the eyes of excecuted prisoners. This was the first time a cataract was described as the lens of the eye and the first time people were aware that the cataract was something that could be removed.
First extracapsular cataract extraction • 1748 – The first extracapsular cataract surgery by Jacques Daviel of Paris. • Required a very mature cataract surrounded by liquid cortex. • Incision was half way around the circumference of the cornea. Since there were no stitiches, the patient was immobilized with sandbags during healing. Mortality was secondary to pulmonary embolis. • Daviel claims 206 surgeries with 182 successes – he determined the patients who could successfully undergo his surgery – had to have a very mature cataract.
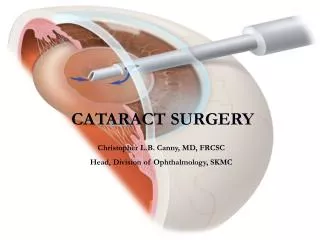
Technique • Daviel created a large cut in the cornea, opened the anterior capsule with a sharp instrument and irrigated the nucleus out. • Cortex – mostly liquid - was removed along with the nucleus. • The posterior capsule was left in place. If cortex was adherent to the capsule, inflammation ensued and the eye was lost.
Intracapsular Cataract Extraction • ICCE was soon developed. Daviel’sextracapsular surgery was too limiting, requiring very mature cataracts. Patients were blind for long periods before their cataract could be removed. Intracapsular surgery allowed lens removal at any stage of the cataract. Intracapsular surgery soon eclipsed Daviel’s surgery, and extracapsular surgery fell into disuse.
Anesthesia • General anesthesia introduced in 1840’s – prior to this patients were secured with ropes and straps for surgery • Topical cocaine was introduced to anesthetize the eye in 1884 • Retrobulbar anesthesia introduced in 1914 • Topical anesthesia again became wide spread in the 1990’s
IgnazSemmelweis (1818-1865) • Hungarian physician on OB ward • Noted doctor’s ward had three times the mortality of the midwives ward – over 35% • Thought it had to do with doctors coming directly to OB ward from morgue dissecting rooms • Advocated handwashing – decreased mortality to less than 1%
A Hero? • Not in his own time – his ideas were only widely adopted after his death • He was committed to an asylum, where he was beaten to death by the guards at age 47 • Louis Pasteur confirmed germ theory years after Semmelweis’ death
1888 Manchester • In Manchester, thousands of cataract surgeries were performed with no gloves, no anesthesia, no drapes, The patient was lying on the table. Only the instruments were sterile.
Intracapsular surgery • Intracapsular surgery involves taking the entire lens out of the eye. Delicate zonules that hold the lens were broken for lens removal. • Initially forceps and suction cups were used to extract the lens. • Ignacio Barraquer (1884-1965) 1917 invented first motorized vacuum instrument (erisophake) for removing the lens • 1957 – Jose Ignacio Barraquer (1916-1998)of Spain introduced alph-chymotrypsin – an enzyme to dissolve zonules • 1961 –TadeuszKrawicz of Poland used cryosurgery to remove the cataract with a tiny probe attached by freezing it to the cataract • 1976 – hyaluronate acid introduced to maintain the anterior chamber
1940’s • Harold Ridley began working on intraocular lenses in England. He noted shattered fragments from airplane canopies lodged in the eyes of WWII Spitfire pilots. He realized these fragments were inert and caused no inflammation in the eye. He created the first intraocular lenses for this material – polymethylmethacrylate. The first IOL was placed by Harold Ridley in 1950.
A Hero? • Ridley performed his surgeries late at night with only his most trusted nurse assisting – when discovered he had implanted lenses, he was ostracized • Only late in his life was he recognized for his immense contribution to cataract surgery
Intraocular lenses • Iris clip lenses and anterior chamber lenses allowed intraocular correction of refractive error. • These lenses allowed efficient, comfortable rehabilitation. Gone was the discomfort of contact lenses and the distortion of aphakic lenses.
Peter Choyce created the first intraocular lens in the USA – first FDA approved lens - in 1981 • Very controversial – Duke-Elder wrecked Peter Choyce’s career for this
Extracapsular cataract surgery • Preserving the posterior capsule and zonules created a safer, more stable platform to secure the intraocular lens. It also decreased the risk of retinal detachment and macular edema following surgery. • This procedure still required a large incision to remove the lens and place the IOL • Initially, the lenses were limited to patients over 65 since long term stability was unknown
The first posterior implants (the kind we use today) made their appearance in the 1980’s. Material and insertion techniques have changed as materials improve and ideas innovate.
PMMA lenses • Made from polymethylmethacrylate • First widely used lenses • Rigid design, single piece • Requires large incision due to rigid nature, so not used in routine surgery at this time • Still used in some specialty surgery – glaucoma, sew-in lenses
Charles Kelman • In the late 1960’s Charles Kelman of New York developed a technique for emulsifying the lens using ultrasonic vibrations and aspirating the emulsified cataract. This technique, called phacoemulsification, combined ultrasound, irrigation, and aspiration to create a closed chamber surgery, allowing small wounds and safer surgery. It did not gain widespread acceptance until the 1990’s.
Phacoemulsification • Phacoemulsification allows us to take cataracts out through small incisions. It created a demand for intraocular lenses that could be placed through a small incision.
Silicone lenses • Now on third generation silicone – a more stable compound • First foldable lens • Long track record • One of the mostly commonly usedlenses today
Acrysoft lens • Versitile– safe in all patients • One piece design, acrylic material • Safe for all retinal patients (DM, s/p RD, expected retina surgery in future-especially with silicone oil) • Problems – expense -negative dysphotopsia • Benefit – does not interfere with vitrectomy surgery
ACRYSOF® Natural IOL Filters high-energy UV AND Blue Light – this slight yellow color of the lens is thought to be protective for macular degeneration.
ReSTORlens One piece design, Acrylic material Concentric ring design but more sophisticated that the ReZoom lens Center targets reading (allows reading in bright light - large pupil diminishes this and focuses primarily at distance in dim light) Drawbacks – halos at night - poor contrast sensitivity - negative dysphotopsias
Crystalens Hinged lens, allowing lens to move forward with accomodative effort Controvertial if it indeed works or how long it works No glare or halos Final position in eye varies due to hinged design, therefore, final refaction can vary – on average 1/3 of patients with this lens require a second surgery to focus them at distance
Correcting Astigmatism Astigmatism occurs when the cornea is not perfectly spherical. It is typically corrected with glasses or contact lenses. With cataract surgery, astigmatism can be corrected by two ways – lateral relaxing incisions (LRI’s) and the toric IOL. LRI’s are paired cuts on the cornea that help round the cornea, making it more spherical. Each person heals differently and, althoughtLRI’s work, they are inexact. They also contribute to dry eye problems from the additional corneal surgery. Toric IOLS are very precise in the astigmatism range they are available. Their main drawback is price. The Toric Intraocular lens