Predictors of Buprenorphine-Naloxone Dosing in Opioid-Dependent Youth: A 12-Week Trial Analysis
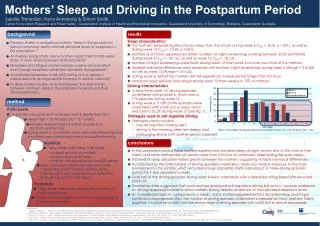
This study examines baseline characteristics that predict buprenorphine-naloxone dosing in opioid-dependent youths. In a 12-week NIDA Clinical Trials Network study with 69 participants aged 15-21, researchers explored how sociodemographic factors, levels of pain, and withdrawal symptoms influenced dosing. Findings reveal that youth reporting "extreme" pain required higher doses compared to those with "some" pain or no pain. Notably, baseline pain did not predict poorer treatment outcomes, indicating that while pain may elevate medication needs, it does not adversely affect addiction treatment effectiveness.

Predictors of Buprenorphine-Naloxone Dosing in Opioid-Dependent Youth: A 12-Week Trial Analysis
E N D
Presentation Transcript
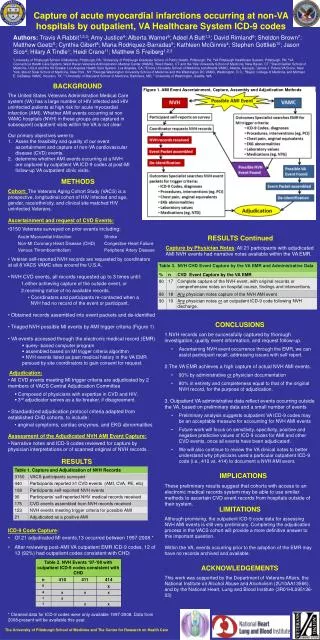
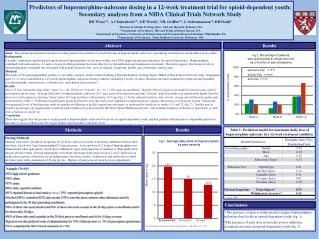
Predictors of buprenorphine-naloxone dosing in a 12-week treatment trial for opioid-dependent youth: Secondary analyses from a NIDA Clinical Trials Network Study RD Weissa,b, A Chakrabartia,b, GE Woodyc, ML Griffina,b, G Subramaniamd, DR Dodda a Division of Alcohol & Drug Abuse, McLean Hospital, Belmont, MA b Department of Psychiatry, Harvard Medical School, Boston, MA c Department of Psychiatry, University of Pennsylvania and Treatment Research Institute, Philadelphia, PA d Department of Psychiatry, Johns Hopkins University, Baltimore, MD Abstract Results Aims: The present investigation examines baseline patient characteristics to predict dosing of buprenorphine–naloxone, a promising treatment for opioid addiction in youths. Background Currently, methadone and the partial opioid agonist buprenorphine are the most widely used FDA-approved pharmacotherapies for opioid dependence. Buprenorphine, combined with naloxone in a 4:1 ratio to lower its abuse potential, has been effective for detoxification and maintenance treatment. Research suggests that dosing levels in opioid dependence treatment are associated with patient-related factors: race, psychiatric symptoms, gender, and, potentially, chronic pain. Methods This study of 69 opioid-dependent youths is a secondary analysis of data collected during a National Institute on Drug Abuse (NIDA) Clinical Trials Network study. Outpatients aged 15–21 were randomized to a 12-week buprenorphine–naloxone dosing condition (including 4 weeks of taper). Baseline measures examined to predict dosing included sociodemographic characteristics, substance use, and clinical characteristics. Results Most (75.4%) reported having either “some” (n = 40, 58.0%) or “extreme” (n = 12, 17.4%) pain on enrollment. Reports of level of pain were similar for heroin users and for prescription opioid users. Average daily dose of buprenorphine–naloxone (19.7 mg) received by patients reporting “extreme” pain at baseline was significantly higher than the dose received by patients reporting “some” pain (15.0 mg) and those without pain (12.8 mg) (fig. 1). In the adjusted analysis, only severity of pain and withdrawal significantly predicted dose (table 1). Withdrawal significantly predicted dose because this study used withdrawal symptomatology (among other factors) to titrate the dosing. During the dosing period, level of baseline pain made no significant differences in illicit opioid use outcomes, as measured by urinalysis at weeks 4, 8, and 12 (fig. 2). Neither pain at baseline nor dosing was significantly correlated with withdrawal (as measured by the Short Opiate Withdrawal Scale), with baseline frequency of heroin or opioid use, or with years of heroin or opioid use. Conclusion These data suggest that the presence of pain predicts buprenorphine–naloxone dose levels in opioid-dependent youth, and that patients with pain have comparable opioid use outcomes to those without pain, but require higher buprenorphine–naloxone doses. Methods Results Dosing Methods Patients were told to abstain from opioids for >6 hours and to be in mild or moderate withdrawal before their first dose, which was 2 mg buprenorphine/0.5 mg naloxone. A second dose of 2-6 mg of buprenorphine was administered when appropriate, based upon withdrawal, signs and symptoms of sedation or other medication-related adverse events. Dosing adjustments were made following observation on days 2 and 3 and based on medication response (substance use including urine toxicology results), withdrawal, and medication-related adverse events with a maximum of 24 mg per day. Reports of pain were not used for dose adjustments. • Sample (N=69) • 52% high school graduates • 74% white • 57% male • 86% daily cigarette smokers • 61% reported heroin as their main problem; 39% reported prescription opioids • Alcohol (48%), cannabis (62%) and cocaine (39%) were the most common other substances used by participants in the 30 days preceding enrollment • 79% of those who used alcohol and 89% of those who used cocaine in the 30 days prior to enrollment used it for fewer than 10 days • 56% of those who used cannabis in the 30 days prior to enrollment used it for 10 days or more • Injection was the preferred route of administration for 55% of heroin users vs. 7% of prescription opioid users • 72% completed the full 12-week treatment (n = 50) Conclusions • The presence of pain at intake predicts higher buprenorphine–naloxone dose levels in opioid-dependent youth (fig. 1). • The presence of pain does not predict poorer addiction treatment outcomes in opioid-dependent youth (fig. 2).