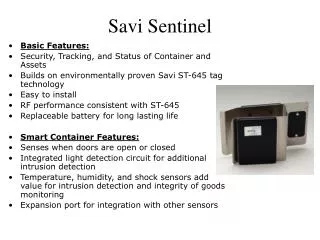
Sentinel Nodes
Sentinel Nodes. J.R.Buscombe RFH. Sentinel Nodes. Uses the Morton principle of logical lymph drainage from a tumour Methods use include blue dye and radiotracers Combination of 2 may be best Pioneers in breast Morton/Krag/Guilianno USA (EIO, Italy and AMC, Netherlands)

Sentinel Nodes
E N D
Presentation Transcript
Sentinel Nodes J.R.Buscombe RFH
Sentinel Nodes • Uses the Morton principle of logical lymph drainage from a tumour • Methods use include blue dye and radiotracers • Combination of 2 may be best • Pioneers in breast • Morton/Krag/Guilianno USA • (EIO, Italy and AMC, Netherlands) • In Melanoma-Morton/Guilianno • May replace high morbidity axillary clearance
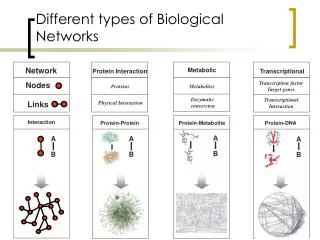
Sentinel nodes Tumour 2nd and 3rd order nodes Sentinel (1st node)
Morbidity of Axillary Surgery • Seroma 50% • Lymphoedema 10-30% • Severe ICBN neuralgia 5% • Shoulder-girdle dysfunction 20% • Numbness 80% Lymphoedema rates: RT alone : 10% Sampling: 10% Level III clearance 30% Surgery + RT: 70%
Sentinel nodes • Methods all similar • Depends on injecting radiotracer in or near cancer • Using gamma camera and probing to track tracer through lymphatics • Intra-operative probe to remove the sentinel node
Sentinel node • Controversies • Who to inject • Where to inject • How much to inject • How much activity to inject • What colloid to use • When to operate • Training
Injection technique isstandardised: IntradermalPeriareolar,tumour quadrant Different injection sites (intradermal, subareolar and peritumoural) have advantages and disadvantages depending on the desired effect on the pattern and kinetics of lymphatic drainage. NEWSTART is designed to minimise visualisation of IMN • Activity injected will depend on the time from injection to surgery • Massage post injection
Size matters • The size of a colloid may have an effect on its transit • However not simple as charge and flexibility of the colloid may change transit • Remember the lymph system is a complex transit system and may be affected by many factors
What size then? • No perfect colloid for sentinel node scintigraphy • All colloids designed for another job • Nanocol – infection imaging • Albures – lymphoscintigraphy • MAA – lung scanning
How colloids made? • Normally made from albumin • Man • Cow • Pig • Often heated to form clusters • May be spun • Can vary in size by factor of 10
Types of colloids used • Tc-99m antimony colloid • 3-30 nm • Tc-99m sulphur colloid-filtered • 50-100 nm • Tc-99m HSA-nanocoll • 4-100 nm • Tc-99m HAS Albures • 200-2000 nm • Tc-99m MAA • >5000nm
Optimal colloids • Will pass to sentinel node and stay there • Smaller colloid will pass through so multiple nodes seen • May clear form sentinel node totally so no counts if >4 hours post injection • Frequent imaging helps
Intra-operative probing • If using small colloids should be done within 4 hours post injection • Larger colloids can be done at 24 hours • During imaging mark site of sentinel nodes on the skin in two planes • External probing can help pre-op
Intra-operative probing • About 20 different probe types available • Different crystals have different sensitivities • Most use CdTe, CsI, NaI BiGeO crystals • Needs good collimation to prevent activity passing through the side of the probe
Intra-operative probing • Inject blue dye at site of tumour just before operation • Use blue dye to help find lymphatics • Probe along blue dye tract until signal high • Remove node send to histology
Sentinel nodes • Results • Pagenelii’s group from Milan • Over 400 patients 98% successful identification of sentinel node • Caution from USA (Krag et al) High variability in results surgeon to surgeon (64-100% PPV) • Issues of training/audit ALMANAC
Potential problems • Injection incorrect (intradermal) • Breast not massaged • Colloid too small/big (manafcturer’s QC) • Probing performed badly so node missed • Poor collimation means signal swamped • Problems with histology etc
Areas where problems seen in breast cancer • Multifocal/centric tumours (maybe helped by nipple injection) • Find this disease with Tc-99m MIBI or MRI • Previous surgery around primary • Breast irradiation • Neo-adjuvant chemotherapy • Vascular invasion of tumour
Sentinel nodes • Can it replace axillary clearance as a staging procedure • Need to await phase III trials • Patients with T1N0 randomised to ax clearance or sent node • Who has better morbidity • Any difference in survival • Need 5 year follow-up
Results in Melanoma • Published by Morton’s group • Reviewed results of 1900 patients having sentinel node for melanoma • All had blue dye and colloid • All had Breslow thickness greater than 5mm • Recurrence rate measured at a mean of 7 years
Does sentinel node effect outcomes? • Morton’s review • Ann Sur Onocol 2000 • 1900 patients • Sentinel node vs blind wide local excision
How is melanoma sentinel node different? • Melanoma can occur anywhere • Drainage much more variable • May drain to more than one set of nodes • Head and neck • Trunk • Different speeds of flow • Leg 20-30 minutes • Head 60-120 minutes
Method-melanoma • Normally done after removal of primary • Aim to identify correct block of lymph nodes to disect • Inject at 4 pints around scar of excision • Inject at least 5mm away from the scar • Massage gently • Image draining nodes • Calf-groin • Back Both inguinals and both upper thorax
Melanoma-methods • Mark any node found • Use shadow gram and laterals and obliques help surgeon identify node • In op use blue dye to find lymphatics and direct surgeon to node • Surgeon the removes sentinel and associated nodes
Melanoma in the leg In leg passage fast up into groin, as the groin nodes are the draining nodes the sentinel node is in the groin The popliteal nodes are ignored
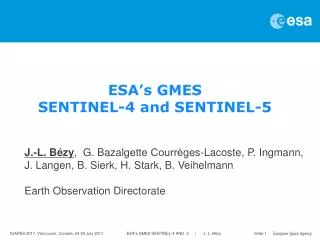
Melanoma on crest of head covered by lead; note bilateral sentinel nodes
Other sites in which sentinel node can be used • Melanoma – all patients as variable drainage • Penis • Tongue • Head and neck • Vulva • Colon!
NEW STARTSLN training programme 2004-2006 Joint Project • Department of Education: Royal College of Surgeons of England • Cardiff University Wales Supported by • DoH, National Assembly in Wales • GE Healthcare • BNMS
NEW STARTSLN training programme National Training Programme • Standardised methodology and training materials • Focus on multidiscipline team – Surgery,Nuclear medicine/physics, Radiology, Theatre nurses, Pathology, etc • Experienced validated training teams • Unique workplace training and mentorship • Quality assured • Centrally audited and validated (anonymised data collection)
NEW START SLN training programme: Standardized National Training • World wide trials* have shown ad-hoc adoption of SLNB, with little formal training, reduces the accuracy of SLN identification for the first 50 procedures. • Evidence from the UK ALMANAC trial demonstrates that structured training shortens the learning curve to less than 10 procedures. * Cox et al: Annals Surg. Oncol.1999, vol l6, page 6
NEW START SLN training programme Overview 3 training phases 1.Theory Day In House Training Validation Stand alone SLNB Theory Skills SLNB + standard procedure Projected Time frame:18-24 months
Conclusion • Sentinel node study established in melanoma and breast • Useful in reducing mutilating surgery • Simple to learn technique but needs good colloid and good probe • Can be combined with other NM test such as PET and scintimammography • All members of the team important