Rural Hospital Safe Practices Program Recommendations
This program offers alternative recommendations for rural hospitals to meet safe practice standards without significant financial investment in CPOE systems. Recommendations focus on non-technology approaches and emerging technologies like smart pumps and automation equipment.

Rural Hospital Safe Practices Program Recommendations
E N D
Presentation Transcript
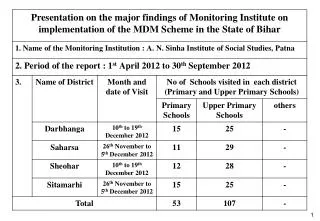
Safe Practices Program: Rural Texas Medical Institute of Technology CPOE • Recommendation Summary • The task force felt that the current CPOE Leap requirement was beyond the financial capability of the greater majority of rural facilities. The task force reviewed the following recommendations from the MHA and agreed that these were reasonable and acceptable alternatives to implementation of a CPOE system in the rural setting. • Recommendation Details • In view of the feedback received from the MHA and those front line rural hospital providers in our research test bed the following recommendations are offered: • Allow credit to rural hospitals that have implemented a robust set of performance improvement activities that could substitute to meet the safe practice without large capital investments. Incorporate the following non-technology approaches into the criteria for measurement of Action responses to the survey question and provide credit for use of any three or four alternatives. • Non-technology approaches: • Use an adverse drug event trigger tool, perform a root cause analysis and track progress • Implementation of a policy on a ‘Do not use’ abbreviation list. (JCAHO) • Implementation of a policy on checking two patient ID’s prior to medication administration, e.g.Pt DOB, Med Rec# (JCAHO) • Use of pre-printed orders that incorporate clinical guidelines, particularly with high-risk medications. • Ensure program is in place for staff and patient education on medication continuity (medication across settings) and implementation of a medication reconciliation process with the patient through all phases of the hospitalization from admission through discharge. (JCAHO) • Completion of an ISMP Survey and development of a medication safety action agenda based on results. • Ensure 24 hour pharmacist is available onsite, on-call, or on-line and provide structured support (e.g. software or internet based medication safety program) to qualified clinical staff to compliment the responsibilities of the pharmacy department when not on site including a process to monitor policy compliance. • Use of a medication registry for adverse events related to meds e.g. MedMarx, MedWatch. OR Use of a tool which tracks all reported medication errors, in the context of a Just Culture of safety promoting reporting. • Use information from the Minnesota Adverse Health Care Event Reporting Law: Care Management event or other similar state data bases where available. • Due to the complexity of implementing alternative systems to achieve the impact of a CPOE system, additional questions should be built into this section of the survey that address specific lower technology approaches for hospitals that are making proactive choices allowing credit for commitment to implement either of these technologies within 12-18 months of completion of the survey: Technology Approaches: • Implementation of automated medication dispensing equipment that has patient profiling capability. • Use of bedside scanning/ barcode-enabled point-of-care (BPOC) identification; this can be the final safety check before medication reaches the patient. • Smart pumps were seen by several as an emerging technology that has the potential to reduce many Intravenous medication related adverse drug events that are presently slipping through the system. It potentially requires a capital investment and research into the appropriate smart pump system for each facility but is an emerging technology being considered.