Download
1 / 1
10 likes | 213 Vues
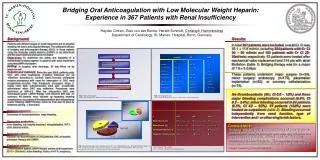
Bridging Oral Anticoagulation with Low Molecular Weight Heparin: Experience in 367 Patients with Renal Insufficiency. Heyder Omran, Giso von der Recke, Harald Schmidt, Christoph Hammerstingl Department of Cardiology, St. Marien- Hospital, Bonn, Germany . Background:

E N D
Bridging Oral Anticoagulation with Low Molecular Weight Heparin: Experience in 367 Patients with Renal Insufficiency Heyder Omran, Giso von der Recke, Harald Schmidt, Christoph Hammerstingl Department of Cardiology, St. Marien- Hospital, Bonn, Germany Background: Patients with different stages of renal impairment are at elevated bleeding risk due to anticoagulant therapy. The safety and efficacy of bridging oral anticoagulant therapy (OAC) in those patients using low molecular weight heparins (LMWH) is not determined and the exact treatment protocol is not stated. Objectives: To determine the safety and feasibility of a standardized bridging regimen in patients with renal impairment using the LMWH enoxaparin. Setting: In hospital; after discharge, 30 day follow up by telephone call. Patients and methods:Since the year 2000, patients under OAC with renal insufficiency (Creatine Clearance [Cr Cl] <50ml/min according to Cockroft Gault Formula) undergoing invasive procedures with need for interruption of OAC were prospectively enrolled. Half- therapeutic enoxaparin doses (1 mg/kg once daily subcutaneously) were peri- procedurally administered when OAC was ineffective. Procedures were performed at INR<1.5. After the intervention OAC was reintroduced under LMWH therapy until effective INR was re- achieved. All patients were followed up regarding bleeding complications, occurrence of thromboembolism and other adverse events following LMWH-therapy, follow up time was 30 days by telephone call (fig. 1, flow chart). Results: In total 367 patients were included, overall Cr Cl was 35.1 ± 11.8 ml/min, including 264 patients with Cr Cl 30 – 50 ml/min and 103 patients with Cr Cl 20- 30ml/min, respectively. 53 patients were treated after mechanical valve replacement and 314 pts with atrial fibrillation (table 1). Bridging therapy was for a mean of 7.6 ± 5.2 days. These patients underwent major surgery (n=34), minor surgery/ endoscopy (n=175), pacemaker implantation (n=82), or coronary catheterization (n=76). No thromboembolic (0%; CI 0.0 – 1.0%) and three major bleeding complications occurred (0.8%, CI 0.2 – 2.4%); minor bleeding occurred in 24 patients (6.5%, CI 4.2 – 9.5%). 51 patients (13.9%) were treated as outpatients (table 2). Bleeding occurred independently from renal function, type of intervention and / or other single risk factors. overall AF MVR n 367 314 53 CHADS 2 --- 2.5±1.2 --- Cr Cl [ml/min] 35.1±11.8 35.1±11.9 37.3±9.2 age [years] 80.8±6.7 81.1±6.5 78.7±5.9 gender [m/f] 147/220 124/190 23/30 therapy [days] 7.6±5.2 7.6±5.5 7.3±4.2 hypertension [n] 295(80.4%) 261(83.1%) 34(64.2%) diabetes [n] 28(7.6%) 14(4.5%) 14(26.4%) embolism [n] 100(27.2%) 90(28.7%) 10(18.9%) CHF [n] 108(29.4%) 90(28.7%) 18 (33.9%) discontinuation of OAC • therapy with LMWH • inclusion/exclusion criteria • informed consent Risk stratification / assessment of renal function halftherapeutic LMWH-dosage (enoxaparin 1mg/kgKG/24h) Follow-up (30 day by telephone call) (total bloodcount, platlet count, bleeding, embolism) Fig. 1 flow chart registry (OAC = oral anticoagulation; LMWH = low molecular weight heparin) Tab.1 demographic data (CrCl = creatinine clearance; m= male; f = female; CHF = chronic heart failure) overall Cr Cl CrCl 30-50ml/min 20-30ml/min n367 264 103 Minor bleeds [n] 24 (6.5%, CI 4.2 – 9.5%) 13 (4.5%, CI 4.2 – 9.5%) 11 (10.7%, CI 4.2 – 9.5%) Major bleeds [n] 3 (.5%, CI .2 – 2.4%) 2 (.8%, CI .01 – 2.7%) 1 (.97%, CI .02 – 5.3%) Thromboembolism [n] 0 (0%; CI 0.0 – 1.0%) 0 (0%; CI 0.0 – 1.4%) 0 (0%, CI .02 – 5.3%) Outpatient treatment [n] 51 (13.9%) 43 (16.3%) 8 (7.8%) Subgroup MVR MtVR Primary endpoints: Occurrence of thromboembolism, major bleeding. Secondary endpoints: minor bleeding, out- hospital treatment, rehospitalization, HIT II, other adverse events. Inclusion criteria: Indication for discontinuation of OAC; effective OAC at hospital admission; therapy with LMWH. Exclusion criteria: Contraindication against LMWH therapy; severe renal impairment (Cr Cl < 20ml/min); active bleeding; history of HIT II, pregnancy. AVR DVR intermediate risk * MVR AF Conclusions: Bridging- therapy using reduced doses of enoxaparin in patients with renal impairment was safe and effective in a large cohort of patients, without need for laboratory monitoring of LMWH- activity. This approach did not increase thromboembolism and led to a low incidence of major bleeding complications. high risk AF Fig.2 treatment groups after stratification for TE- risk. Intermediate risk = AF and CHADS2 score 2. (AF= atrial fibrillation; MVR= mechanical valve replacement; MtVR= mitral valve replacement; AVR= aortic valve replacement; DVR= double valve replacement) TE = thromboembolism;) Tab.2 Results; *p = <0.05 (Cr Cl = creatinine clearance; CI= confidence interval)