Immunosuppressive Drugs
280 likes | 934 Vues
Immunosuppressive Drugs. Immune System Module. The immune system is designed to protect the host from invading pathogens and to eliminate diseases, while retaining the capacity to recognize "self" antigens to which it is tolerant. Protection from infection and diseases is provided

Immunosuppressive Drugs
E N D
Presentation Transcript
Immunosuppressive Drugs Immune System Module
The immune system is designed to protect the host from invading pathogens and to eliminate diseases, while retaining the capacity to recognize "self" antigens to which it is tolerant. • Protection from infection and diseases is provided • by the innate and the adaptive immune system. • This adaptive response culminates in the production • of antibodies which are the effectors of humoral immunity and the activation of T-lymphocytes which are the effectors of cell-mediated immunity.
Immunosuppressive drugs: • Agents that suppress the immune system play an important role in retention of organs transplants and tissue grafts and in the autoimmune diseases, while preventing the patient from becoming immunologically compromised.
They are classified according to their mechanisms of actions into: • Selective inhibitors of cytokine production and function. • Antimetabolites affecting cell metabolism; preventing lymphocytic proliferation. • Mono and polyclonal antibodies that block T cell surface molecules.
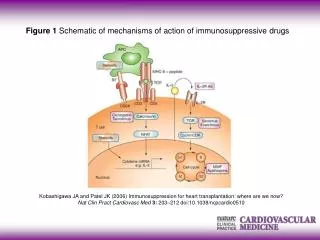
1-Selective inhibitors of cytokine production and function: • Cytokinesinclude interferon (IFNs), interleukins (ILs), tumor necrosis factors (TNFs), colony stimulating factors and transforming growth factors. IL-2 is of a special importance as it stimulates the proliferation of T-helper cells which produce more IL-2, IFN-Y and IFN-B. • These cytokines activate NK cells, macrophages and cytotoxic T- lymphocytes. • Examples: cyclosporin, tacrolimus.
Cyclosporin • -Used to prevent rejection of allograft transplants. It is more effective when used with glucocorticoids, although can • be used alone. • -Can be used in treatment of autoimmune diseases as rheumatoid arthritis and uveitis.
Mechanism of action: • It affects mainly cell-mediated immunity, to a lesser extent humoral immunity. It binds with cyclophilin (a member of a class of IC proteins called immunophilins) to form a complex which inhibits calcineurin that is necessary for activation of a T-cell- specific transcription factor NFATc. This factor is involved in synthesis of interleukins including IL-2→decreased number of IL-2 which is the main stimulus of increasing T lymphocyte's number.
Adverse effects: • Nephrotoxicity is the most common and is potentiated by concomitant administration of nephrotoxic drugs such as aminoglycosides and NSAIDs.
II- Immunosuppressive antimetabolites: • Azathioprine: • It is a prodrug which is converted first to 6-MP then to thioinosinic acid which interferes with purine synthesis at steps required for lymphoid cell prolioferation that follows antigenic stimulation. • The main toxic effect is bone marrow depression usually manifested as leukopenia which is increased by co-administration of ACEIs or cotrimoxazole. • Other antimetabolities: Mycofenolate mofetil.
III-Antibodies: • These are either polyclonal antibodies (variable and less specific) directed against a number of lymphocyte antigen or monoclonal AB (homogenous and more specific). • Examples: antithymocyte globulins & Muromonab-CD3.
Antithymocyte globulins: • They are used mainly with other immunosuppressants to treat the hyperacute phase of allograft rejection. They are polyclonal, when bind to surface of circulatory T lymphocytes various reactions occur →impaired T cell responses. • Adverse effects: These mostly associated with injection of a foreign protein. Anaphylaxis, serum sickness, leukopenia, thrombocytopenia, viral infections and lymphoma.
IV-Adrenocorticoids: • Prednisone or methyl prednisolone most commonly used for transplantation. Steroids are used in acute rejection of solid organ allografts and in chronic graft-versus-host syndrome. • Also, are used for auto immune diseases, e.g. rheumatoid arthritis and SLE.
Mechanism of action: • -Decrease generation of cytokines; • Decrease concentration of complement • also inhibit the functions of tissue macrophages and other antigen-presenting cells. • Interferes with antigen expression from the grafted tissue, delay revascularization . • interferes with the sensitization of cytotoxic T- lymphocytes and the generation of AB-forming cells.
Adverse effects: • Iatrogenic Cushing syndrome (in most patients who are given daily doses of 100 mg of hydrocortisone or more or the equivalent amount of synthetic steroid for longer than 2 weeks).Adrenocortical suppression (thus, must be gradually withdrawn), diabetes, hypertension, peptic ulcer, osteoporosis, cataract, glaucoma, mood and behavioural changes; salt and water retention and hypokalemia;and increased liability for infections.