Download
1 / 74
740 likes | 1.1k Vues
Reproductive Endocrinology Related Diseases 生殖内分泌相关疾病. Zhejiang University School of Medicine, Women ’ s Hospital Wu Ruijin. Reproductive Endocrinology Related Diseases. Dysfunctional Uterine Bleeding 功能失调性子宫出血(功血) Amenorrhea 闭经 Polycystic Ovarian Syndrome ( PCOS ) 多囊卵巢综合征

E N D
Reproductive Endocrinology Related Diseases生殖内分泌相关疾病 Zhejiang University School of Medicine, Women’s Hospital Wu Ruijin
Reproductive Endocrinology Related Diseases • Dysfunctional Uterine Bleeding 功能失调性子宫出血(功血) • Amenorrhea 闭经 • Polycystic Ovarian Syndrome(PCOS) 多囊卵巢综合征 • Premenarche Syndrome(经前期综合征 ) • Perimenopause Syndrome(围绝经期综合征 ) • Hyperprolactinemia(高催乳激素血征 )
Mechanism of Normal Menses ▷下丘脑-垂体-卵巢轴(hypothalamic-pituitary-ovarian axis,HPOA)调节和反馈正常 ▷卵巢正常(有足够始基卵泡和对Gn正常的反应性) ▷子宫完整,子宫内膜对雌、孕激素有正常反应性 ▷下生殖道通畅
Abnormal Uterine Bleeding (AUB) Any bleeding that deviated from regular, cyclic (28+/- 7 days) bleeding of normal amount (≤80ml) and duration (2-8 days). • Includes abnormal menstrual bleeding and bleeding due to other causes such as pregnancy, systemic diseases, or cancer. • The diagnosis and management present some of the most difficult problems in gynecology. • In childbearing women, a complication of pregnancy must always be considered, and more than one entity may be present, eg, uterine myomas and cervical cancer.
异常子宫出血(一) 周期 经期 经量 规则 延长 过多 (> 7天) (>80ml) 规则 正常 过多 不规则 延长 过多 不规则 可延长 不太多 月经过多 (menorragia) 经量过多 (hypermenorrhea) 子宫不规则过多出血 (menometrorrhagia) 子宫不规则出血 (metrorrhagia) • Menorrhagia: Excessive uterine bleeding at regular intervals • Metrorrhagia: bleeding between regular menstrual periods
异常子宫出血(二) 月经频发(polymenorrhea):周期少于21天。 月经稀发(oligomenorrhea):周期长度超过35天。 月经过少(hypomenorrhea):月经稀疏,出血少于2天。 接触性出血(contact bleeding):性交后出血,排除宫颈癌等。 Polymenorrhea: Irregular bleeding at infrequent intervals
Dysfunctional uterine bleeding (DUB)功能失调性子宫出血(功血)
Definition Abnormal bleeding without clear anatomic cause. 调节生殖的神经内分泌机制失常引起的异常子宫出血,无全身及内外生殖器质性病变。
Anovulatory dysfunctional uterine bleeding (无排卵性功血)(85%) Puberty(20%): unstable HPOA regulation with growing follicle but no LH peak and ovulation does not occur. Perimenopause (50%):ovary becomes low responsive to Gn and its function declines. Child bearing period(30%):inside/outside interference, such as psychologic factor, environment, stress,etc. Pathogenesis
Anovulatory (1)breakthrough bleeding(雌激素突破出血): 子宫内膜受单一E刺激而无孕酮对抗引起; (2)withdrawal bleeding(雌激素撤退出血 ): 子宫内膜在单一E的刺激下持续增生,因一批卵泡闭锁 导致E,内膜失去E支持剥脱出血。 内膜过厚,脆性↑ 内膜修复困难 血管结构功能异常 子宫内膜出血自限性机制缺陷 局部因子异常:PGs 凝血、纤溶异常
Ovulatory menstrual dysfunction (排卵性月经失调)(15%) Luteal phase defect (LPD) (黄体功能不全) Abnormal FSH/LH or ratio, low LH peak or following pulse defect. Irregular shedding of endometrium(子宫内膜不规则脱落) HPOA dysfuction and corpus luteum degenerate uncompletely
Anovulatory Endometrial hyperplasia (子宫内膜增生症):1994, WHO simple hyperplasia (单纯型增生 ) complex hyperplasia (复杂型增生 ) atypical hyperplasia (不典型增生) Proliferative phase endometrium (增生期子宫内膜) Atrophic hyperplasia(萎缩型子宫内膜) Ovulatory menstrual dysfunction LPD :P↓→分泌期腺体分泌不良 Irregular shedding of endometrium (子宫内膜不规则脱落):P低量持续→不规则脱落,混合型 Pathology
Anovulatory Symptoms: Irregular uterus bleeding (metrorrhagia) Characteristic of bleeding: (1)irregular cycle and duration (2)not stop by oneself (3)irregular amount (4)no menalgia (痛经) (5)anaemia “三不一无一贫” Clinical Findings
Ovulatory menstrual dysfunction • Luteal phase defect (LPD) (黄体功能不全) (1)shorten cycle, luteal phase <11d, frequently cycle (2)infertility (3)repeating spontaneous abortion (4)D & C:luteal phase endometrium defected and backward 2d to standard phase • Irregular shedding of endometrium(子宫内膜不规则脱落) (1) prolonged and heavy menses (2) D & C: proliferative and secretary endometrium coexist in cycle d5 (3)BBT high temperature phase prolonged to next menstruation (4) Serum E2,P and BBT,D&G,cervix mucus score help to diagnosis
History Physical examination and pelvic examination Auxiliary examination (1)Blood/live/clotting function test (2)HCG (3)Endometrial biopsy /Dilatation and Curettage (D&C):stop bleeding and pathologic diagnosis (4)Ultrasound or Hysteroscopy: exclude intracavity diseases (5)Ovulation function examination (6)Others: cervical cytologic examination Diagnosis
Ovulation function examination 1. B ultrasound detects follicles and ovulation 2. BBT (基础体温测定) 3. Vagina cells smear 4. Cervical mucus score (宫颈粘液评分) 5. Endometrial biopsy 6. Serum hormone: E2, P 7. Urine and serum LH 8. Laproscope
2.基础体温测定 双相体温
Low E2 state High E2 state
Insler宫颈评分法 -- ―――――――――――――――――- -- -- 项目评分 0 1 2 3 粘液量 无 颈管内 颈管口见粘液 溢出宫颈口 拉丝度 无 <4 cm 4~10 cm >10 cm 结晶 无 少量细条状 羊齿状 典型结晶 宫颈口 闭 裂隙 部分开放 开张(瞳孔样) --――――――――――――――――――――― 宫颈粘液拉丝度
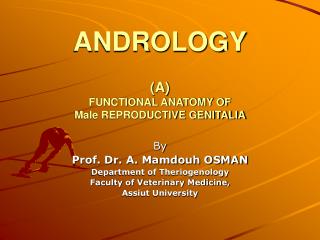
Proliferative Endometrium (增生期子宫内膜) Secretory Endometrium (分泌期子宫内膜)
Pregnancy related diseases Hemorrhagic diseases Genital tract diseases Endocrinal diseases Drugs Differential Diagnosis
General treatment: antiinflammatory, retrieve anaemia (纠正贫血), enhance nutrition as the time stop bleeding. Drug treatment:hormonal therapy Principle of treatment:(1)stop bleeding,(2) cycle regulation, (3)induce ovulation (or reduce bleeding). (1) stop bleeding (止血): 8h见效、24-48h基本止血,超过96h考虑诊断更改;合理剂量,渐减量,持续无出血20天 。 雌激素:适于无排卵型青春期功血。 常用药物及方法:妊马雌酮、乙烯雌酚、戊酸雌二醇 孕激素:体内有一定E水平,药物性刮宫,甲羟孕酮、炔诺酮 雄激素:增强收缩,单用效差,适于绝经过渡期功血。 联合用药:避孕药、三合激素 Treatment to anovulative DUB
(2)cycle regulation(调整周期): 雌、孕序贯法(人工周期):青春期、生育期,低E2 雌、孕联合法(避孕药):生育期高E2 、绝经过渡期 后半周期法(孕激素):青春期、绝经过渡期 (3) induce ovulation (促进排卵): to women desire bearing children Clomiphene citrate, CC (氯米芬) Human chorionic gonadotropin, HCG (绒促性素) Human menopausal gonadotropin, HMG (尿促性素) Follicle stimulating hormone,FSH (卵泡刺激素), FSH-HP,r-FSH Gonadotropin releasing hormone agonist, GnRHa (促性腺激素释放激素激动剂)
Operation treatment: Diagnosis Curettage: often used in acute heavy bleeding or exist high risk of endometrial cancer Endometrial ablation(子宫内膜切除术): Peri-menopause heavy bleeding, hormone therapy does not work and no child-bearing request Hysterectomy(子宫切除术): medicine therapy does not work and patient choose
Induce follicles development — CC, HMG+ hCG, Ergolactin (溴隐停) Promote LH peak — hCG 5000-10000U Increase luteal function — progestogen, 10mg Induce luteal resolve —progestogen Treatment to menstrual dysfunction
Amenorrhea 闭 经
Definition • primary amenorrhea(原发性闭经):5% No period by age 16 regardless of the presence of normal growth and development or the appearance of 2nd sexual characteristics.(≥16岁,第二性征已发育,尚无月经来潮;) 或 No period by age 14, absence of growth or development of 2nd sexual characteristics;(≥14岁,无第二性征,无月经来潮) • secondary amenorrhea(继发性闭经):95% No period for a length equivalent to at least 3 x previous cycles intervals or no periods for 6 months. (月经停止6个月,或自身3个周期以上)
Classification • Classic • Hormonal (1) Gonadotropins(按FSH水平分) ▷高FSH闭经:血清FSH>30IU/L,提示卵巢功能衰退 ▷低FSH闭经: FSH、LH<5IU/,提示病变在下丘脑或垂体 (2)Estrogen(按雌激素水平分) ▷Ⅰ度闭经:子宫内膜已受一定雌激素影响,用孕激素后有撤退性出血(黄体酮试验) ▷Ⅱ度闭经:体内雌激素水平低落,子宫内膜菲薄或萎缩,用孕激素后不出现撤退性出血 (3)Prolactin:高泌乳素血症 • “4- Compartment” (按解剖部位分) Outflow tract——Ovary——Anterior pituitary——Hypothalamus 中枢神经-下丘脑-垂体-卵巢-子宫
Pathogenesis Primary Amenorrhea (原发性闭经) • 多由遗传学原因或先天性缺陷引起 • 体内有一定雌激素水平则第二性征发育正常或接近正常 • 体内无雌激素分泌第二性征缺乏
Secondary Amenorrhea 继发性闭经 1.Hypothalamic amenorrhea下丘脑性闭经(55%): 最常见, 功能性为主,GnRH 脉冲分泌频率、幅度、量的异常均可致闭经。 ①精神应急性(psychogenic stress) :创伤、紧张、环境改变 ②体重下降、神经性厌食(weight loss,anorexia nervosa) ③长期 过剧运动 : 体脂减少 Leptin下降 ④药物: 可逆性 利血平、氯丙嗪 下丘脑多巴胺 垂体PRL 避孕药 抑制下丘脑GnRH ⑤颅咽管瘤: 瘤体压迫垂体柄,下丘脑GnRH和多巴胺运送受抑制 ⑥Kallmann综合征(嗅觉缺失综合症) • 下丘脑GnRH先天性分泌缺陷伴有嗅觉丧失或减退 • 低促性腺激素性性腺功能减退 • 原发闭经、无性征发育、内生殖器分化正常
2. Pituitary Amenorrhea 垂体性闭经(20%): ① hypophyseal tumor(垂体肿瘤):催乳激素细胞肿瘤,致闭经溢乳综合征 ②hypophyseal infarct (垂体梗死)(Sheehan syndrome): 由于产后出血和休克导致垂体急性梗塞和坏死,使腺垂体丧失正常功能引起一系列腺垂体功能低下的症状,包括: 产后无乳、脱发、低促性腺激素闭经, 生殖器官萎缩,以及肾上腺皮质、甲状腺功能减退症状如低血压、畏寒、嗜睡等。 ③empty sella syndrome(空蝶鞍综合征):蝶鞍隔破坏,蛛网膜下腔向蝶鞍延伸,蝶鞍充满脑脊液
3. Ovarian amenorrhea 卵巢性闭经(20%) • XO syndrome or absence (先天性性腺发育不全或缺如):Turner’s syndrome • premature ovarian failure,POF(卵巢早衰) • Ovaries histoclasia or resection (卵巢组织破坏或切除) • Ovaries functional tumor (卵巢功能性肿瘤) • polycystic ovary syndrome, PCOS(多囊卵巢综合征)
性腺先天性发育不全 占原发性闭经35% 性腺发育不全 、卵泡缺如、性征幼稚、雌激素水平低下, 属高促性腺激素闭经, 75%染色体异常,25%染色体正常 ①染色体异常 最常见Turner’s syndrome X染色单体45,XO:性腺发育不全、第二性征发育不良; 特殊体型:身材矮小(<150CM),盾胸、蹼颈、后发际低; 继发性闭经见于嵌合体45, XO/46XX,或X短臂、长臂缺失等 ②单纯性腺发育不全(染色体正常) 46,XX 条索状性腺 46,XY 条索状性腺(Swyer综合征)
对抗性卵巢综合征: • 卵巢具有始基卵泡和初级卵泡,形态饱满 • 卵巢对FSH不敏感,可能存在FSH受体缺陷 • 卵泡无分泌雌二醇功能,血FSH升高 • 女性第二性征接近正常,女性维持性征的雌激素来自卵巢间质在高LH刺激下产生雄烯二酮外周转化
POF: 定义: 在40岁以前出现的高促性腺激素(FSH≥40IU/L)伴随低性激素水平(E2≤30pg/ml),临床表现为原发或继发闭经。 发生率: Coulam 检查1858例POF,发现40岁妇女1/100发生POF,30岁1/1000 原发闭经POF 10%~28% 继发闭经POF 4%~18% 病因: • 卵泡耗竭:卵泡起源数缺乏,卵泡闭锁加速 • X染色体异常 • 半乳糖血症 • 卵泡功能紊乱:酶缺陷,讯号缺陷 • 免疫作用
4.Uterine amenorrhea 子宫性闭经(5%) Congenital absence of uterus 先天性无子宫或发育不全(米勒管发育不全综合征) ▷染色体46,xx,内分泌正常,有排卵,第二性征正常 ▷无子宫、无阴道,少部分始基子宫 ▷宫内胚胎发育副中肾管中、尾段未发育 子宫内膜损伤:如Asherman syndrome 子宫内膜炎症:结核性、感染 手术或腔内放疗 5.Congenital hypogenital dysplasia 先天性下生殖道发育异常:处女膜闭锁、阴道缺如 6. Pathocrinia 其它内分泌功能异常:甲低、甲亢等
Diagnosis (etiological diagnosis) • History: exclude pregnancy for secondary amenorrhea • Physical examination and pelvic examination • Auxiliary examination
评估雌激素水平 宫颈评分法 阴道脱落细胞检查 孕激素试验阳性为I度闭经 雌激素试验 方法:雌孕激素序贯试验 有撤退性出血为II度闭经 重复试验仍无撤退性出血为子宫性闭经
子宫功能测定 子宫内膜活检 子宫输卵管碘油造影(HSG) 宫腔镜 药物撤退性试验 卵巢功能测定 BBT B超监测卵泡 激素测定:E2、P(>15.9nmol/l,提示有排卵),T; FSH>40IU/L提示卵巢功能衰竭 宫颈评分法 阴道脱落细胞检查
垂体功能测定 ▷垂体兴奋试验(GnRH刺激试验): 静脉注射GnRH刺激垂体,观察血FSH和LH变化 垂体功能正常者刺激后30分钟比基值升高2-4倍 反应低下或无反应—垂体功能减退 反应亢进-PCOS ▷激素:PRL<25ug/L、FSH、LH ▷头颅X片、CT 其它检查 : 染色体,甲状腺,肾上腺功能,腹腔镜,宫腔镜等