Download

1 / 71
790 likes | 1.6k Vues
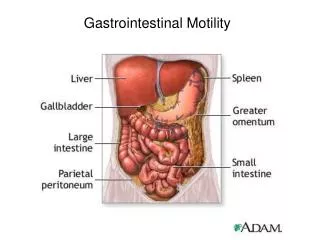
Gastrointestinal disorder. ISLAMIC University Nursing College . Gastrointestinal Tract. GI tract consists of a hollow muscular tube starting from the oral cavity, going through the rectum and is ended at the anus, where food is expelled.

E N D
Gastrointestinal disorder ISLAMIC University Nursing College
Gastrointestinal Tract • GI tract consists of a hollow muscular tube starting from the oral cavity, going through the rectum and is ended at the anus, where food is expelled. • Main function GI is turning food into nutrients which can be absorbed by the human body to provide energy needed for survival • Accessory organs that assist the tract by secreting enzymes to help break down food into its component nutrients (salivary glands, liver, pancreas and gall bladder)
Gastrointestinal Tract: Assessment • Health history • Gestational age and birth weight. • Nutritional history (length of BF, introduction of solid food). • Neonatal & infancy GI problems. • Family factors (life style, hereditary problems. • present changes in child’s life (start schooling, new sibling or death in the family) • Assessment of the digestive function in a 24hr (food intake and elimination)
Gastrointestinal Tract: Physical Exam • physical parameter (Wt and Ht) • Skin Color • Inspection of oral cavity • S & S of dehydration • Abdominal and rectal assessment • Peristalsis • Abdominal Tenderness • Distended abdomen • Displaced heart (diaphragmatic hernia) • Hair (loss of pigment or brittle)
Gastrointestinal Tract: Problems • Regurgitation(spitting-up) • Vomiting. • Mechanical due to obstruction • Reflexive due to infection or allergy • Central due to CNS involvement (meningitis) or sepsis • Vomitousassessment includes: • Onset & frequency • Quantity • Degree of forcefulness • Presence of bile
Gastrointestinal Tract: Problems • Abdominal distention may be due to: • Accumulation of fluid or gases • Congenital malformation • Constipation • Hernia • GI perforation • Cirrhosis • Abdominal pain
Gastrointestinal Tract: Problems • Diarrhea • Acute due to: • Infection. • Stress. • Drug reaction. • Chronic due to: • Chronic infection • Malabsorption • Obstruction inflammatory bowel disease.
Gastrointestinal Tract: Problems • Assessment of Diarrhea • Onset • Frequency • Consistency & Quantity • Odor, presence of blood mucus • Combining factors (food, medication ..etc)
Gastrointestinal Tract: Diagnostic tests • CBC, ESR, Electrolytes • Liver enzymes • Pancreatic enzymes (amylase) • Bilirubin • Serum ammonia • Stool testes • Stool culture/occult blood • Stool fat • Stool pH
Gastrointestinal Tract: Diagnostic procedures • Gastric Analysis • Specimen is taken using NG tube • pt should be NPO after midnight • Stomach contents are examined for: • Hydrochloric acid • Occult blood • Malignant cells • Bacteria/parasites
Gastrointestinal Tract: Diagnostic procedures • Barium Swallow • Visualize esophagus, stomach and duodenum in upright position behind fluoroscopic screen • Pt should be NPO after midnight • Post-care • Encourage fluid intake to prevent constipation • White stools up to 72 hrs
Gastrointestinal Tract: Diagnostic procedures • Barium enema • Examining rectum and colon • Assist in the diagnosis of • Tumor • Polyps • Defects associated with Crohn’s and ulcerative colitis diseases • Preparation • Water enema to clear colon and rectum • NPO
Gastrointestinal Tract: Diagnostic procedures • Endoscopy • Visualize the upper and lower GI by fiberoptictube.
Gastrointestinal Tract: Diagnostic procedures • Colonoscopy • Visualize large intestine • Diagnosis of constipation/diarrhea, anorexia, rectal bleeding, pain, polyps and tumors • Preparation • NPO (8 hrs) • Laxative a few days prior • Enema the night before the procedure • Post • Cramps due to air in the colon • Abdominal distention, bleeding
Gastrointestinal Tract: Nursing Care • Monitoring • Caloric intake • Daily wt • Abdominal girth • Intake and output • Stool chart • Help family for lifetime adjustment to the disease by; • Encouraging early family involvement in child’s care • Educating family about the consequence of GI alteration on child’s health and life style ( decrease oral gratification and availability of energy for mobility
Cleft Lip & Cleft Palate • Incomplete fusion of the embryonic structure surrounding the primitive oral cavity • Among the most common facial anomalies • Genetic basis is present (family history for presence of the defect in other siblings) • Incidence rate of cleft lip is 1:7800 • Incidence rate of cleft palate alone in 1:2000 • May result in communication between the nasal and oral cavities
Cleft Lip & Cleft Palate • Cleft lip may be unilateral or bilateral • Cleft lip may be accompanied with cleft palate • Cleft palate may be present without cleft lip (non-visible): early sign is dripping milk from nose
Cleft Lip & Cleft Palate • Assessment should be focused on; • In newborn: compromised sucking ability • Respiratory status • Family reaction
Cleft Lip & Cleft Palate • Management • Surgical repair for cleft lip during the first few weeks of life • Initial repair for cleft palate during 4-6 months of age and the surgical correction between 6-18 months
Cleft Lip & Cleft Palate • Nursing care • Provide adequate nutrition and prevent aspiration and infection (otitis media) • During feeding • Upright position • Feed slowly • Burp frequently
Cleft Lip & Cleft Palate • After the surgical operation • Restrains may be necessary to prevent disturbance of the surgical site • No straws, tooth brushing • Prevent infection • follow-up assessment of • Growth • Speech • Teeth development
Cleft Lip & Cleft Palate • Complications • Makes sucking weaker: altered nutrition • Speech difficulties • May affect development of teeth and jaw • Affect the bite • More frequent ear infection
Cleft Lip & Cleft Palate • Nursing diagnosis: • Altered nutrition related to physical defect / difficulty eating • Risk for aspiration • Risk for infection • Risk for impaired verbal communication • Altered family process
Hypertrophic Pyloric Stenosis • An overgrowth of the circular muscle of the pylorus, results in obstruction/ partially / narrowing of the pyloric sphincter • Cause is unknown, however there is a hereditary component • The stomach contractions increase in frequency and force to empty the stomach content.
Hypertrophic Pyloric Stenosis • Usually develops in the first few weeks of life • Clinical Manifestation: • Regurgitation small amounts of milk immediately after feeding. • Projectile vomiting. • Vomiting may occur during feeding or shortly after feeding • Vomitus contain NO bile • Gastritis due to prolonged stay of stomach content • Wt loss and dehydration • Metabolic alkalosis • Failure to thrive
Hypertrophic Pyloric Stenosis • Assessment • Olive-like mass at right epigastrium under the edge of the liver. • Peristaltic waves can be noted after feeding moving from left to right. • Ultrasoundgraphy. • Treatment is by surgery: to allow better passage of milk.
Hypertrophic Pyloric Stenosis • Nursing diagnosis: • Fluid volume deficit. • Nursing Care: • Monitor intake and output. • Assess vomitus. • Prevent dehydration. • Monitor Wt and Ht.
Intussusception • Is an invagination of part of the intestine into an adjacentdistal portion of the intestine. • Occurs in healthy infants around 6 months of age and rarely occur before 3 months or after 3-years of age • More common in male infants • The cause is unknown. • The most common type is near the ileocecal valve pushing into the cecum and onto the colon.
Intussusception • The involved intestine become inflamed and edematous with bleeding from the mucosa • Untreated intussusception can lead to intestinal gangrene, peritonitis and death • Diagnosis by barium enema ( if there is intraperitoneal air from a bowel perforation thus enema is contraindicated)
Intussusception • Assessment is focused on: • Stool inspection (currant-jelly stools) • CM such as Pain • Abdominal palpation
Intussusception • Early symptoms • Crampy abdominal pain and a drawing up of the knees to the chest • periods of apathy • Poor feeding and vomiting • Late symptoms • Worsening vomiting, becoming bilious • Abdominal distension/ Palpable abd. Mass (sausage-shaped) • Heme positive stools • Followed by “currant jelly” stools: Jelly stools due to leaking of blood and mucus into the intestinal lumen as a result of venous engorgement • Dehydration • If untreated, necrosis and perforation are possible
Intussusception • Treatment • Supportive therapy (Fluid; Antibiotics) • Hydrostatic barium • Operation • Manual • Resection and reanastamosis
Hirschsprung’s Disease (aganglionic megacolon) • A congenital anomaly resulting from an absence of ganglion cells in the colon (lack of nerve ending in the sigmoid colon) • Autosomal dominant genetic mutataions • More common in male & children with down syndrome • peristalsis can not occur
Hirschsprung’s Disease (aganglionic megacolon) • CM • Newborn: • failure to pass meconium after birth (during the firs t 24 hr) • Poor feeding and spitting up • Visible bowel loops • Bile-stainedvomitus • Abdominal distention • Infancy • Failure to thrive • Constipation & Abdominal distention • Diarrhea & vomiting/ Explosive watery stool • fever
Hirschsprung’s Disease (aganglionic megacolon) • CM • Childhood (more chronic: • constipation • Ribbon-like & foul smelling stools • Abdominal distention • Palpable fecal masses • Poorly nourished • Lethargy, nausea and anorexia • Treatment by surgery (removal of non-motile part) • Colostomy/ileostomy care after surgery • After surgery high fiber diet is established • Prevent enterocolitis
Celiac Disease • A disease of malabsorption & abnormal immune reaction to gluten • Celiac disease is a hereditary intolerance of gluten (protein found in wheat, barely, oats, rye) • Gluten protein (gliadin) causes inflammation and damages villi in the small bowel • Enzyme insufficiency (peptidase) causes accumulation of toxic gluten peptide • Gluten toxicity results from alteration in immunologic response • It is the second cause of malabsorption after CF
Celiac Disease • CM (related to malabsorption and malnutrition) • Problem starts after the introduction of solid food • Diarrhea; Steatorrhea (stool is bulky, fatty foul smelling) • Wt loss (due to poor absorption of protein, CHD, vit and iron) • Weakness; Abdominal pain & distention • Bone & joint pain • Anemia (malabsorption of iron) • Vit. Deficiency • Failure to thrive ( without S&S of GI problems) • Behavioral changes: irritability, apathy and uncooperative
Celiac Disease • Assessment • Family history • Child’s dietary history • Diagnostic test • anti-tissue transglutaminase antibodies (tTGA) or anti-endomysium antibodies (EMA). • Malabsorption test • CBC • Biopsy of jejunal (atrophy of villi) • Serum protein & immunoglobulin decreased
Celiac Disease • Dietary management • a gluten-free diet • In acute phase; • corticosteroid • fluid replacement • N/G to decrease the distention
Celiac Disease • Family education: • Diet regimen: free of wheat and barley • Monitor growth and development • Complications (if not treated) • Iron deficiency anemia • Osteoporosis • infertility or recurrent miscarriage • depression or anxiety • tingling numbness in the hands and feet • seizures
Inflammatory bowel diseases: Ulcerative colitis & Crohn’s disease • Inflammatory bowel disease (IBD) refers to chronic conditions that cause inflammation in some part of the intestines. • The intestinal walls become swollen, inflamed, and develop ulcers • IBD can cause discomfort and serious digestive problems • Symptoms depend on which part of the digestive tract is involved