Download
1 / 78
910 likes | 1.27k Vues
Cardiac Muscle and Organ Mechanics. Roy Kerckhoffs Dept of Bioengineering, University of California, San Diego Tutorial on heart and lungs Ohio State University, Columbus, OH, 20 sep 2006. Outline. Ca 2+. Ca 2+. Ca 2+. k n. R off. R off. 0. *. k b. Ca 2+. *. k off. k on. R on.

E N D
Cardiac Muscle andOrgan Mechanics Roy Kerckhoffs Dept of Bioengineering, University of California, San Diego Tutorial on heart and lungs Ohio State University, Columbus, OH, 20 sep 2006
Outline Ca2+ Ca2+ Ca2+ kn Roff Roff 0 * kb Ca2+ * koff kon Ron Ron 0 * g g f Ca2+ 0 A1 A1 * Ca2+ system system organ organ tissue tissue cell cell
Overview • Anatomy and physiology of the heart • System and organ level • Resting cardiac tissue • Active force generation: the sarcomere • Multi-scale modeling • Anatomic models • Models of cardiac mechanics: from cell to system • Models of cardiac electromechanics
Cardiac Anatomy Mitral SVC Aorta Pulmonary artery Pulmonic Tricuspid valves Base LA RA LV RV Septum Epicardium Endocardium Apex
Pericardium Vaw Vra Vla Vrv Vlv Vperi Vvw • A sac wherein the heart sits • Limits sudden increases in volume • Increases atrio-ventricular and ventricular-ventricular interaction *Freeman & Little, AJP 1986;251:H421-H427
Physiology of the heart Conduction System right atrium sinusnode left atrium AV-node left bundle branch right bundle branch left ventricle Purkinje fibers right ventricle
The Cardiac Cycle 2 1 3 4b 4a • Systole: • 1. Isovolumic contraction • 2. Ejection • Diastole: • 3. Relaxation • Early • Isovolumic • 4. Filling • a) Early, rapid • b) Late, diastasis 4a 4b 1 3 2
Pressureand Volume 2 3 4b 1 4a 1 6 AVC 1 4 1 2 Aorta AVO 1 0 Pressure (kPa) 8 6 4 Left ventricle 2 MVO MV C 0 1 5 0 1 2 0 Volume (ml) 9 0 6 0 3 0 0 1 0 0 2 0 0 3 0 0 4 0 0 5 0 0 6 0 0 7 0 0 Time (msec)
The Pressure-Volume Diagram End-systole (ES) 2 0 SV=EDV-ESV Ejection Fraction EF=SV/EDV Ejection 1 6 AVC AVO 1 2 Pressure (kPa) Stroke volume (SV) Isovolumic relaxation Isovolumic contraction 8 End-diastole (ED) 4 Filling MVO MVC 0 5 0 1 0 0 1 5 0 2 0 0 0 Volume (ml)
The Pressure-Volume Diagram 2 0 Ejection 1 6 AVC AVO 1 2 Pressure (kPa) Stroke (external) work Isovolumic relaxation Isovolumic contraction 8 4 Filling MVO MVC 0 5 0 1 0 0 1 5 0 2 0 0 0 Volume (ml)
Preload and Afterload 2 0 ESPVR 1 6 control 1 2 Pressure (kPa) preload 8 EDPVR afterload 4 0 5 0 1 0 0 1 5 0 2 0 0 0 Volume (ml)
Time-Varying Elastance E( 20 0) = E max E(1 60 ms ec) VR 2 0 E(1 20 ms ec) ESP 1 6 1 2 Pressure (kPa) E(8 0 m sec ) 8 R EDPV 4 0 0 50 100 150 200 LV Volume (ml) P(t) = E(t){V(t) - V0}
Starling’s Law of the Heart(The Frank-Starling Mechanism) increased contractility (e.g. adrenergic agonist) decreased contractility (e.g. heart failure) Stroke work “Preload” (EDV or EDP)
Contractility (Inotropic State) increased contractility (e.g. adrenergic agonist) 2 0 ESPVR decreased contractility (e.g. heart failure) 1 6 1 2 Pressure (kPa) 8 EDPVR 4 0 5 0 1 0 0 1 5 0 2 0 0 0 Volume (ml)
Physiological Basis of Starling’s Law 2 0 ESPVR 1 6 1 2 Pressure (kPa) 8 EDPVR 4 0 5 0 1 0 0 1 5 0 2 0 0 0 Volume (ml)
Overview • Anatomy and physiology of the heart • System and organ level • Resting cardiac tissue • Active force generation: the sarcomere • Multi-scale modeling • Models of cardiac mechanics: from cell to system • Models of cardiac electromechanics
Minimizing Stress Gradients • Residual Stress • Fiber Angles • Torsion
Resting Tissue Properties • Nonlinearity • Hysteresis • Creep • Relaxation • Preconditioning Behavior • Strain Softening • Anisotropy
Passive Biaxial Properties 1 0 Fiber stress 8 6 Stress (kPa) 4 Cross-fiber stress 2 0 0. 0 0 0. 0 5 0. 1 0 0. 1 5 0. 2 0 0. 2 5 Equibiaxial Strain
Measurement of Myocardial strain • Radiopaque beads and biplane x-ray • video imaging of markers • ultrasound • MRI tagging
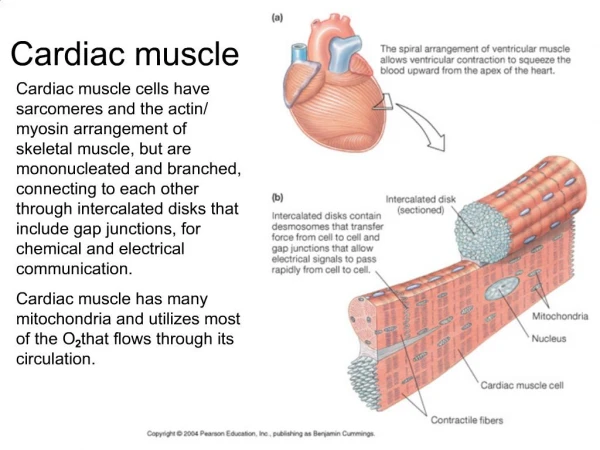
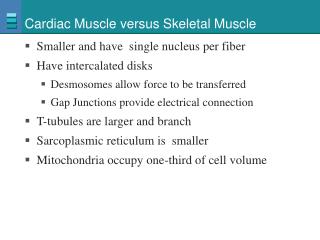
Myocyte Connections • Myocytes connect to an average of 11 other cells (half end-to-end and half side-to-side) • Myocytes branch (about 12-15º) • Intercalated disks • gap junctions
Overview • Anatomy and physiology of the heart • System and organ level • Resting cardiac tissue • Active force generation: the sarcomere • Multi-scale modeling • Models of cardiac mechanics: from cell to system • Models of cardiac electromechanics
Cardiac Myocytes • Rod-shaped • Striated • 80-100 m long • 15-25 m diameter
Striated Muscle Ultrastructure Electron micrograph of longitudinal section of freeze-substituted, relaxed rabbit psoas muscle. Sarcomere shows A band, I band, H band, M line, and Z line. Scale bar, 100 nm. From Millman BM, Physiol. Rev. 78: 359-391, 1998
Excitation-Contraction Coupling • Calcium-induced calcium release • Calcium current • Na+/Ca2+ exchange • Sarcolemmal Ca2+ pump • SR Ca2+ ATP-dependent pump http://www.meddean.luc.edu/lumen/DeptWebs/physio/bers.html
Isometric Tension in Skeletal Muscle:Sliding Filament Theory (a) Tension-length curves for frog sartorius muscle at 0ºC (b) Developed tension versus length for a single fiber of frog semitendinosus muscle
Isometric Testing 700 500 200 300 400 600 100 Sarcomere length, mm Sarcomere isometric 2.1 2.0 Muscle isometric 1.9 Tension, mN 2.0 1.0 time, msec
Length-Dependent Activation 2.2 micrometer 1.6 micrometer Isometric peak twitch tension in cardiac muscle continues to rise at sarcomere lengths >2 mm due to sarcomere-length dependent increase in myofilament calcium sensitivity
Isotonic Testing Isovelocity release experiment conducting during a twitch Cardiac muscle force-velocity relation corrected for viscous forces of passive cardiac muscle which reduce shortening velocity
Ventricular Mechanics: Summary of Key Points • Ventricular geometryis 3-D and complex • Fiber anglesvary smoothly across the wall • Systoleconsists of isovolumic contraction and ejection; diastoleconsists of isovolumic relaxation and filling • Area of the pressure-volume loop is ventricular stroke workwhich increases with filling (Starling’s Law) • Ventricles behave like time-varying elastances • The slope of the end-systolic pressure volume relation is a load-independent measure of contractility or inotropic state.
Ventricular Mechanics: Summary of Key Points (cont’d) • Collagencontributes to anisotropicresting properties • Myocardial straincan be measured invasively and non-invasively • Torsion and residual stress tend to compensate for these gradients in the ventricles to maintain uniform fiber strain
Overview • Anatomy and physiology of the heart • System and organ level • Resting cardiac tissue • Active force generation: the sarcomere • Multi-scale modeling • Models of cardiac mechanics: from cell to system • Models of cardiac electromechanics
Integrative In-Silico Biology Functional Integration, Structural Integration • Functional integration • of interacting physiological processes • Structural integration • across scales of biological organization (c) 2004 Andrew McCulloch, UCSD
Why modeling • hypothesis generation • clinical applications • diagnosis • training platforms for surgeons • predict outcomes of surgical interventions • predict outcomes of therapies
Why multiscale modeling • Cardiac structure and function are heterogeneous: most pathologies are regional and non-homogeneous • Ca2+ important ion in electrophysiology and responsible for cardiac force generation • Many interacting subsystems in basic processes: e.g. • ventricular stress coronary flow • electrical activation mechanical activation (ECC and MEF) • feedback of baroreceptors on cardiac contractility and frequency
Overview • Anatomy and physiology of the heart • System and organ level • Resting cardiac tissue • Active force generation: the sarcomere • Multi-scale modeling • Models of cardiac mechanics: from cell to system • Models of cardiac electromechanics
Models of cardiac mechanicscellular • Development of models of cellular cardiac mechanics have lagged behind models of cellular cardiac electrophysiology, due to • lack of available solving algorithms (and computer power) • controversies about basic mechanisms of force generation in myofilaments • 4 categories: • phenomenological time-varying elastance models (algebraic) • phenomenological Hill-models (ODE) • A.F.Huxley type models of crossbridge formation (PDE) • Landesberg type myofilament activation model (ODEs)
Modeling Myofilament Force Production • Ca2+ binding to TnC causes tropomyosin to change to a permissive state • Force development occurs as actin-myosin crossbridges form • Crossbridges can ‘hold’ tropomyosin in the permissive state even after Ca2+ has dissociated
Myofilament Activation/Crossbridge Cycling Kinetics Ca2+ Ca2+ Ca2+ kn Roff Roff 0 * kb Ca2+ * koff kon Ron Ron 0 * g g f Ca2+ 0 A1 A1 * Ca2+ Non-permissive Tropomyosin koff Permissive Tropomyosin f Permissive Tropomyosin, 1-3 crossbridges attached (force generating states) Ca2+ not bound to TnC Ca2+ bound to TnC This scheme is used to find A(t), the time-course of attached crossbridges for a given input of [Ca2](t)
Myofilament Model Equations • Total force is the product of the total number of attached crossbridges, average crossbridge distortion, and crossbridge stiffness:
Myofilament model: results 0 * Noff Noff 0 * Roff Roff * 0 Non Non 0 * Ron Ron 0 * A1 A1 µtitin 0 * A2 A2 Factive µgel ηcell 0 * A3 A3 Myofilament model of active force generation + Passive mechanics of single myocyte Model validation experiments • Simultaneous measurement of intracellular Ca2+ and shortening in single myocytes
Nonlinear Elasticity of Soft Tissues • Soft tissues are not elastic — stress depends on strain and the history of strain • However, the hysteresis loop is only weakly dependent on strain rate • It may be reasonable to assume that tissues in vivo are preconditioned • Fung: elasticity may be suitable for soft tissues, if we use a different stress-strain relation for loading and unloading – the pseudoelasticity concept • a rationale for applying elasticity theory to soft tissues • Unlike in bone, linear elasticity is inappropriate for soft tissues; we need nonlinear finite elasticity
Models of cardiac mechanicstissue • Passive • strain energy functions • orthotropic (fiber – crossfiber – sheet) • heterogeneous • Active • orthotropic (fiber – crossfiber – sheet?) • heterogeneous(!) (Cordeiro et al, AJP 286, H1471-H1479, 2004)
Models of cardiac mechanicsorgan • Solve tissue models on anatomy with e.g. finite element or finite difference method • Compute part of cardiac cycle, e.g. produce Frank-Starling curves, or • Compute full cardiac cycle with coupling to circulatory model