Download
1 / 24
240 likes | 563 Vues
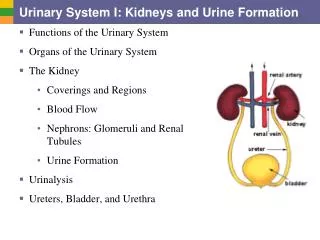
Urinary catheters, I & O and 24 hour urine testing. PN 103. Catheters - may be used for intermittent or continuous drainage -may be introduced into the bladder, ureter, or kidney -type and size determined by location and cause of the urinary tract problem

E N D
Catheters • - may be used for intermittent or continuous • drainage • -may be introduced into the bladder, ureter, or • kidney • -type and size determined by location and cause • of the urinary tract problem • -measured by the French system • -Urethral catheters range in size from 12Fr-24Fr • -Ureteral catheter: 4FR-6Fr and always inserted by • the physician
Types of Catheters • -Coude’ -tapered tip, easier to insert when • enlarged prostate is suspected • -Foley -simple uretheral catheter, balloon near the • tip to anchor • -Malecot, Pezzer, or Mushroom –used to drain • urine from the renal pelvis of the kidney, can also • be used for suprapubic drainage • -Robinson –a straight catheter with multiple openings in the • tip to facilitate intermittent drainage • -Ureteral –long, slender catheter passed into the • ureter • -Whistle-tip –has a slanted, larger opening at its tip • to be used if blood is in the urine
Coude’ catheter • Robinson catheter • Ureteral catheter
-Cystostomy, Vesicostomy or suprapubic • catheter –inserted by the physician through • the abdominal wall above the symphysis • pubis; used to divert urine flow from the • urethra, is connected to a sterile closed • drainage system. • -External (Texas or condom0 catheter – • -drainage system connected to the penis • -noninvasive • -removed daily for cleaning and skin • inspection
Nursing Interventions and Patient Teaching • -Principle to prevent and detect infection and • trauma • Aseptic technique for insertion • Record I & O • Adequate hydration • Do not open drainage system after it is in place • except to irrigate the catheter per MD order. • Catheter care twice a day, inspect insertion site • Check system daily for leaks • Avoid placing the drainage bag above the level • of the bladder!
Prevent tension on the system of backflow • wile transferring patient • -Ambulate the patient or turn and • reposition every 2 hours • -Observe characteristics of the urine • -Sterile specimen collected through the • drain port • -Report and record assessment findings
Self-Catherization • -Uses for spinal cord injury or other • neurological disorders • -Promotes independent function of the • patient. • -Instruct about surgical asepsis, however • at home there is less risk of cross- • contamination and patient will probably • use a modified clean technique • -Instruct in symptoms of UTIs
INTAKE AND OUTPUT • One of the most basic methods of monitoring a client's health is measuring intake and output , commonly called I and O. By monitoring the amount of fluids a client takes in and comparing this to the amount of fluid a client puts out. The health care team can gain valuable insights into the client's general health as well as monitor specific disease conditions. I & O
INTAKE- all those fluids entering the client's body such as water, ice chips, juice, milk, coffee and ice cream. Artificial fluids include: parenteral, central lines, feeding tubes, irrigation and blood transfusion.OUTPUT- all fluid that leaves the client's body such as: urine, perspiration, exhalation, diarrhea, vomiting, drainage from all tubes and bleeding. I & O
Ideal Daily fluid Intake and OutputSource/ AMOUNT/ Route/ AMOUNTH2O consumed as fluid/ 1500ml/ urine/ 1400-1500mlH2O present in food/ 750ml / insensible losses/ 350-400mlH2O produced by oxidation/ 350ml / lungs/ 350-400mlskin / 100mlsweat/ 100-200mlfeces /TOTAL/ 2600ml/ TOTAL/ 2300-2600ml I & O
Purpose:- helps evaluate client's fluid and electrolyte balance- suggests various diagnosis- influence the choice of fluid therapy- document the client's ability to tolerate oral fluids- recognize significant fluid losses I & O
Mandatory for clients with burns, electrolyte imbalance, recent surgical procedure, severe vomiting or diarrhea, taking diuretics or corticosteroids, renal failure, congestive heart failure, NGT, drainage collection device and IV therapy. I & O
Deviations:Other sources of fluid loss and excessive losses from normal routes:- drainage from catheter or tubes- vomitus- diarrhea- diaphoresis- hemorrhage- ileostomy/ colostomy drainage- excessive urine output I & O
Average daily water requirement by age and weight:AGE/ ml/ BODY WEIGHT ml/kg3 days/ 250-350ml/80-1001 year/ 1150-1300ml/ 120-1352 years/ 1350-1500ml/ 115-1254 years/ 1600-1800ml/100-11010 years/ 2000-2500ml/70-8514 years/ 2200-2700ml/ 50-6018 years/ 2200-2700ml/40-60adult /2400-2600ml/ 20-30 I & O
Nursing Intervention:Intervention/ Rationale1. Ideally intake and output should be monitored/ To obtain an accurate record2. In critical situations, intake and output should be monitored on an hourly basis/ Urine output less than 500ml in 24 hours or less than 30cc/hour indicates renal failure3. Daily weights are often done/ Indicate fluid retention or loss4. Identify if patient undergone surgery or with medical problem / May affect fluid loss5. Make sure you know the total amount and fluid sources once you delegate this task/ To get an accurate measurement
6. Record the type and amount of all fluids and describe the route at least every 8 hours7. If irrigating a nasogastric or another tube or bladder, measure the amount instilled and subtract it from the total output/ To get exact amount8. Keep toilet paper out of client urine output/ For an accurate measurement9. Measure drainage in a calibrated container and observe it at eye level.
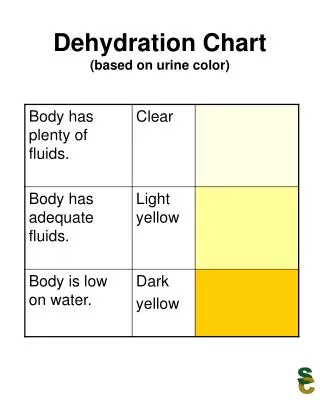
A significant change in a client's weight or a significant difference in a client's total intake and output should be reported immediately to the physician. • WEIGHT CHANGES- mild dehydration- 2 to 5% loss- moderate dehydration- 6 to 9% loss- severe dehydration - 10 to 14% loss- death- 20% loss • mild volume overload- 2% gain- moderate volume overload - 5% gain- severe volume overload - 8% gain
Clinical Signs of Dehydration:- dry skin and mucous membranes- concentrated urine- poor skin turger- depressed periorbital space- sunken fontanel- dry conjunctiva- cracked lips- decreased saliva- weak pulse
Client's signs of fluid excess:- peripheral edema- puffy eyelids- sudden weight gain- ascites- rales in lungs- blurred vision- excessive salivation- distended neck vein
24 hr. Urine – The kidneys excrete substances at various rates and amounts during a 24 hr. period. • Some substances that are measured are: urine protein, urine creatinine, uric acid levels, and catecholamines + 66 other items • Procedure: • Discard the first voiding of the day. • Start the “time” for the 24 hr. collection • Collect urine x 24 hrs.
Collection- remind patient not to place toilet paper in collection container. Have patient void before BM to avoid contamination. • -if there is a preservative in the • collection container, may need to • refrigerate or put on ice. If no • preservative, may need to • refrigerate or put on ice. Check • with the lab and for any • institutional procedures.