Download
1 / 33
410 likes | 970 Vues
Red Blood Cells Disorders. Objectives: To study the features and causes of anemia due to blood loss, hemolysis and defects in red cells production; To learn the features and causes of polycythemia; To study the age-related changes in the red cells of neonates and aging.

E N D
Red Blood Cells Disorders • Objectives: • To study the features and causes of anemia due to blood loss, hemolysis and defects in red cells production; • To learn the features and causes of polycythemia; • To study the age-related changes in the red cells of neonates and aging
Red Blood Cells Disorders • Expected Learning Outcomes: • After learning this topic, students: • are able to describe the pathophysiological mechanisms of anemia due to blood loss, hemolysis and defects in red cell production ; • can describe the pathophysiological features and causes of polycythemia • can understand the age-related changes of red cells in neonates and aging
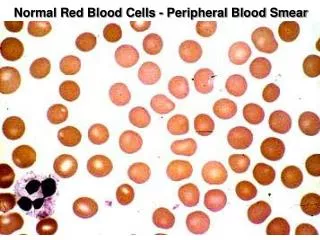
Brief Review of Red Cell Production and Destruction Structure of Hemoglobin
Brief Review of Red Cell Production and Destruction Development of Red Blood Cells
Brief Review of Red Cell Production and Destruction Destruction of Red Blood Cells
Anemia • Abnormally low no. of circulating RBC or low level of hemoglobin (Hb), or both • Resulted from excessive loss or destruction of RBC, or deficient RBC production • Reduced oxygen carrying capacity • Three categories of manifestations: • Impaired O2 transport and the associated compensatory mechanisms • Reduction in red cell and Hb amount • The pathologic process which causes the anemia • Severity dependent
Anemia • Manifestations (cont’d) • Reduced O2 transport tissue hypoxia fatigue, weakness, dyspnea, angina, headache, faintness, dim vision • Redistribution of blood from cutaneous tissues or lack of Hb pallor of skin, mucous membranes, nail beds • Compensatory increase of cardiac output tachycardia, palpitations, ventricular hypertrophy, high-output heart failure (for severe anemia) • Accelerated erythropoiesis bone pain, sternal tenderness • Hemolytic anemia high bilirubin level in blood jaundice • Aplastic anemia is also associated with petechiae and purpura due to reduced platelet function
Anemia • 1. Blood Loss Anemia • Loss of blood and RBC components (e.g. iron) • Acute blood loss – hypovolemia and shock • Hemodilution causes a drop in hematocrit (RBC count) and Hb amount in a blood volume • Hypoxia causes bone marrow to increase RBC production normal hematocrit is restored with few weeks (given that iron reserve is sufficient) • Chronic blood loss – small change in blood volume; more asymptomatic; iron-deficiency anemia if iron reserve is depleted ; microcytic hypochromic anemia if too little functional Hb in RBC
Anemia • 2. Hemolytic Anemia • Premature destruction of RBC • Normocytic (size) and normochromic (pigment) red cells • Hyperactive bone marrow for compensation increase RBC no. • Easy fatigability, dyspnea, jaundice • Intravascular hemolysis – complement fixation in transfusion reactions, mechanical injury, toxins; hemoglobinemia and hemoglobiuria • Extravascular hemolysis – abnormal RBC are destructed in spleen
Anemia • 2. Hemolytic Anemia (cont’d) • Causes - intrinsic and extrinsic to RBC • Intrinsic causes: inherited – defects of cell membrane, hemoglobins and enzymes; hemolysis is resulted • Extrinsic causes: external agents – drugs, bacterial toxins, antibodies, trauma • Inherited Disorders of Red Cell Membrane • Hereditary spherocytosis – deficiency of membrane proteins (spectrin and ankyrin) loss of membrane surface of RBC tight sphere (not biconcave) • Poorly deformable and easily destructed in venous sinuses of splenic circulation • Signs: mild anemia, jaundice, splenomegaly, bilirubin gallstones
Anemia • 2. Hemolytic Anemia (cont’d) • Defects of Hb – Sickle Cell Anemia • Point mutation in chain of Hb to form HbS • Recessive inheritance: ~90% HbS ; heterozygous: sickle cell trait (~40% HbS) • More common in Black American and African (malaria is endemic; protection against Plasmodium falciparum malaria) • Deoxygenated HbS aggregates and polymerizes deformability of RBC (sickled cell) • Consequences of sickling: • Chronic hemolytic anemia – destruction of RBC due to nondeformable membrane • Blood vessel occlusion – sickled cells adhere to endothelial cells endothelial activation release of activator substances (e.g. interleukins, thrombin) hypercoagulation thrombosis
Anemia • 2. Hemolytic Anemia (cont’d) • Defects of Hb – Sickle Cell Anemia (cont’d) • Other factors contributing to sickling: cold, stress, physical exertion, infection, hypoxia, dehydration, acidosis • Clinical course • Pain of various body parts and organ failure due to vessel occlusion, hyperbilirubinemia, jaundice, pigment stones in gall bladder, acute chest syndrome (pulmonary infarction associated with shortness of breath, chest pain, cough), swelling of bony parts due to osteomyelitis, stroke • Growth retardation in children • Ischemia in spleen and splenic injury due to congestion, functional asplenia and more susceptible to infection, especially in children
Anemia • 2. Hemolytic Anemia (cont’d) • Defects of Hb – Sickle Cell Anemia (cont’d) • Laboratory test: hemoglobin electrophoresis, prenatal diagnosis of fetal DNA obtained by amniocentesis • Management: patients are advised to avoid situations that precipitate sickling episodes – e.g. cold exposure, infections, physical exertion, acidosis and dehydration • Use of hydroxyurea to promote the synthesis of more HbF and less HbS; use of nitric oxide to regulate vessel occlusion (under investigation) • Bone marrow transplant
Anemia • 2. Hemolytic Anemia (cont’d) • Defects of Hb – Thalassemias • Inherited disorders with defective synthesis of (-thalassemias)or (- thalassemias)chains of Hb • More severe form in homozygous than heterozygous state • Reduced Hb synthesis and imbalanced globin chain production hypochromatic microcytic anemia • Accumulation of oxygen free radicals causes red cell lysis and anemia • The remaining normal globin chains precipitate in red cell precursors in bone marrow impair DNA synthesis and damage red cell membrane • - thalassemias • Severe anemia from 6-9 months; growth retardation if no blood transfusion • Increased hematopoiesis bone marrow expansion, impair bone growth with abnormalities, thinning of cortical bone, more vulnerable to bone fracture
Anemia • 2. Hemolytic Anemia (cont’d) • Defects of Hb – Thalassemias (cont’d) • - thalassemias (cont’d) • Splenomegaly and hepatomegaly due to increased red cell destruction • Iron overload due to dietary absorption and repeated transfusion • Excess iron deposited in vital organs causes organ damage (e.g. heart and liver) • Iron chelation therapy, bone marrow transplantation, stem cell therapy • -thalassemias • Two pairs of genes for -globin synthesis; deletion of 2 genes shows mild hemolytic anemia • Deletion of 3-4 genes lead to unstable aggregates of -chains to form HbH; common in Asians • HbH-individuals show chronic moderate hemolytic anemia • More severe in infants where 4 genes are deleted – formation of Hb Bart’s from HbF
Anemia 16/ 33 • 2. Hemolytic Anemia (cont’d) • Defects of Hb – Thalassemias (cont’d) • -thalassemias (cont’d) • Hb Bart’s has very high O2 affinity can’t release O2 to tissues death of utero or shortly after birth • Transfusion dependent • Inherited Enzyme Defects • Deficiency of G6PD causes hemolytic anemia; X-linked ; expressed only in males or homozygous females • RBC are more vulnerable to oxidants (e.g. drugs, fava beans) Hb to Met-Hb denatured Hb precipated in RBC • Hemolysis occurs in narrow vessels of spleen hemoglobinemia, hemoglobinuria, jaundice • Diagnosed by G6PD assay (testing G6PD enzyme activity in blood)
Anemia • 2. Hemolytic Anemia (cont’d) • Acquired Hemolytic Anemia • Hemolysis triggered by exogenous factors direct membrane destruction of red cells or antibody-mediated lysis • Exogenous factors: various drugs, chemicals, toxins, venoms, infections (e.g. malaria), mechanical factors (prosthetic heart valves, vasculitis) • Obstruction of microcirculation (e.g. intravascular coagulation, thrombotic thrombocytopenic purpura) can traumatize red cells by turbulence and pressure change • Mediated by immune system – autoimmune response or alloantibodies from blood transfusion; diagnosed by direct antiglobulin test (to detect antibodies on red cell surface)
Anemia • 3. Anemias of Deficient Red Cell Production • Iron-Deficiency Anemia • Reduced hemoglobin synthesis and impaired O2 delivery • Iron is recycled through normal turning-over in spleen • Minor loss in feces; dietary uptake mainly from meat; dietary deficiency in vegetarians and children consume cow’s milk • Iron deficiency due to chronic blood loss – menstruation, gastrointestinal bleeding, peptic ulcer, intestinal polyps, hemorrhoids, cancer, excessive aspirin intake • Iron deficiency due to increased demand – pregnancy ( mother’s blood vol., growing fetus), lactation, child growth
Anemia • 3. Anemias of Deficient Red Cell Production (cont’d) • Iron-Deficiency Anemia(cont’d) • Laboratory tests: low MCHC, MCVand hematocrit values, low serum iron level, microcytic and hypochromatic, poikilocytosis (irregular shape), anisocytosis (irregular size) • Manifestations (severity dependent): fatigability, palpitation, dyspnea, angina, tachycardia, pallor, neurological problems (e.g. developmental delay)
Anemia • 3. Anemias of Deficient Red Cell Production (cont’d) • Megaloblastic Anemias • Red cells are abnormally large ( MCV value) with weak membrane; shorter life span • Resulted from abnormal nucleic acid synthesis • Vitamin B12 (cobalamin) and folic acid deficiencies • Vitamin B12-Deficiency Anemia • Vitamin B12 involves in DNA synthesis and maintain proper membrane structure of neurons • Vitamin B12 is found in all foods and dietary deficiency is not common • Defects in pathways for Vitamin B12 absorption cause deficiency
Anemia • 3. Anemias of Deficient Red Cell Production (cont’d) • Megaloblastic Anemias (cont’d) • Folic Acid-Deficiency Anemia (cont’d) • Similar symptoms to vitamin B12 deficiency, but no neurologic manifestations • Dietary deficiency; folic acid found in green vegetables, fruits and meats • Malabsorption disorders of folic acid caused by drugs • Pregnancy increases the demand of folic acid; more common to show deficiency
Anemia • 3. Anemias of Deficient Red Cell Production (cont’d) • Aplastic Anemia • Bone marrow stem cells reduce production of RBC, white blood cells and platelets • Symptoms – weakness, fatigability, pallor, petechiae on the skin, bleeding from nose, gums, vagina, GI tract • Causes – radiation, chemicals (as in chemoradiotherapy), toxins, viral infections • Idiosyncratic to susceptible persons • Therapy – stem cell replacement, blood transfusion • Chronic Disease Anemias • Anemia as a complication of chronic diseases – e.g. tuberculosis, AIDS, osteomyelitis, rheumatoid arthritis, systemic lupus erythematosus • Chronic renal failure deficiency of erythropoietin anemia
24 / 33 Polycythemia • Abnormally high total red blood cell mass with hematocrit > 50% • Relative polycythemia – loss of plasma volume (water deprivation, excessive diuretic intake) • Absolute polycythemia - red cell mass with a rise in hematocrit; primary or secondary • Primary polycythemia (polycythemia vera) • proliferative disorder of pluripotent stem cells of bone marrow; also associated with white cells and platelet counts • Manifestations: • RBC counts, Hb level, hematocrit, viscosity; hypertension, headache
Polycythemia • Primary polycythemia (cont’d) • Manifestations: (cont’d) • Venus stasis – plethoric appearance • Hypermetabolism – night sweats and weight loss • Thromboembolism death • Secondary polycythemia • Physiological increase of erythropoietin - compensation to hypoxia, e.g living at high altitutes; neoplasms • Similar manifestations to primary polycythemia
Age-Related Changes in Red Blood Cells • Fall in red cell count, hematocrit, MCV and Hb conc in neonate – due to reduced red cell production and dilution by increased plasma volume with growth * • Neonatal red cells have shorter life span (50-70 days); more fragile than adult ones • A switch from HbF (higher O2 affinity) to HbA • Physiologic anemia at ~2 months old; no symptoms • Anemia of prematurity in low-birth-weight infants – poor response to erythropotetin; symptoms: apnea, poor weight gain, pallor, decreased activity, tachycardia
Age-Related Changes in Red Blood Cells • 1. Red Cell Changes in the Neonate • Hyperbilirubinemia in the Neonate • During the first week of life – 60% of term and 80% of preterm neonates are jaundiced (increased serum level of bilirubin); usually self-limiting • Due to increased breaking down of red cells and inability of immature liver to conjugate bilirubin • Other possible factors for elevated bilirubin – breast-feeding, hemolytic disease, hypoxia, infections, biliary obstruction, liver disease • Breast milk contains fatty acids which inhibit bilirubin conjugation in neonate liver; promote absorption of bilirubin from duodenum
Age-Related Changes in Red Blood Cells • Hyperbilirubinemia in the Neonate (cont’d) • At risk for a neurologic syndrome: kernicterus – accumulation of bilirubin in brain cells • Unconjugated bilirubin is lipid soluble and can cross the blood-brain barrier • Asphyxia and hyperosmolality can damage the blood-brain barrier and hence increase the bilirubin level in brain • Symptoms may appear 2-5 days (term) or by day 7 (preterm) • Mild manifestations – lethargy, poor feeding, short-term behavioral changes • Severe manifectations – rigidity, tremors, ataxia, hearing loss; long term damages: involuntary muscle spasm, seizures, mental retardation, deafness • Phototherapy – conversion to structural isomer more soluble and excreted; exchange transfusion if unresponsive
Age-Related Changes in Red Blood Cells • 1. Red Cell Changes in the Neonate (cont’d) • Hemolytic Disease in the Newborn (Erythroblastosis fetalis) • Happens in Rh-positive infants whose mothers are Rh-negative (and sensitized) • Anti-Rh antibodies generated by mothers • Results in agglutination and hemolysis severe anemia with compensatory hyperplasia and enlargement of blood-forming organs – spleen and liver of fetus • Impairment of liver function – reduced albumin production massive edema (hydrops fetalis) • Also associated with kernicterus brain damage or death
Age-Related Changes in Red Blood Cells • Hemolytic Disease in the Newborn (Erythroblastosis fetalis) (cont’d) • Methods to decrease the threat to infants (born to Rh-negative mothers): • Prevention of sensitization – use of Rh antibodies within 72hrs of delivery or abortion • Prenatal identification of at risk fetus – fetal Rh phenotyping • Intrauterine transfusion to the affected fetus – replacement of hemolysed with Rh-negative blood and reduce bilirubin level
Age-Related Changes in Red Blood Cells • 2. Red Cell Changes with Aging • The capacity of red cell production changes with age – decline of the no. of progenitor cells (by 50% at age of 65 and by 70% at the age of 75) • Reduced levels of hematopoietic progenitors and hematopoietic growth factors; reduced sensitivity to such factors; poor response to erythropoietin due to inflammatory cytokines with age • Anemia is more severe in elderly with bleeding, chronic infections, chronic inflammatory disorders, malignancy