Download
1 / 19
220 likes | 867 Vues
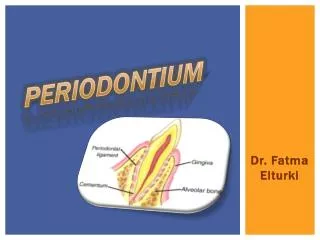
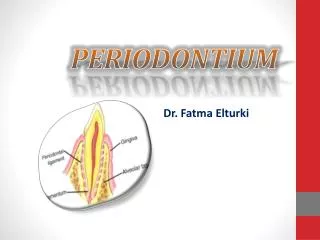
FUNCTIONS OF THE PERIODONTIUM. Attachment & support Nutritive Sensation All components of the periodontium form a FUNCTIONAL SYSTEM that provides attachment for the tooth to the bone of the jaw AND permits the tooth to withstand the forces of mastication.

E N D
FUNCTIONS OF THE PERIODONTIUM Attachment & support Nutritive Sensation All components of the periodontium form a FUNCTIONAL SYSTEM that provides attachment for the tooth to the bone of the jaw AND permits the tooth to withstand the forces of mastication
Principal collagen fibre bundles attach the tooth to the jaw Cementum, PDL and alveolar bone involved in accommodating any tooth movement Teeth held in jaws and supported against functional stresses BUT Allow for tooth movement Intrasocket & Translocatory ATTACHMENT & SUPPORT
All components of PDL act together as a SHOCK ABSORBER Cementum and Alveolar bone respond to stresses at specific sites Ground substance Tissue fluid / blood Fibre bundles of PDL Secretion and resorption Corresponding to areas of tension / compression Physiological tooth movement and PDL
Intra – socket tooth movements • Teeth of opposing jaws come together • - APPLYING FORCE - • Teeth move within sockets • - REMOVING FORCE - • Teeth move back to their original position
Intra – socket movements • Direction and amount of movement depend on direction and amount of force • When force applied – rate of movement rapid initially but DECREASES WITH TIME • - no further movement occurs - • When force removed – rate of movement rapid and DECREASES WITH TIME • - tooth returns to original position -
REMEMBER :– • TOTAL TIME TAKEN FOR A TOOTH TO RETURN TO ITS ORIGINAL POSITION IS GREATER THAN THAT TAKEN TO MOVE UNDER THE IMPOSED FORCE
Physiology during tooth movement OR “whats going on ?” • 3 components of PDL in the system of tooth support • GROUND SUBSTANCE • TISSUE FLUID / BLOOD and BLOOD VESSELS • PRINCIPLE FIBRE BUNDLES • Operate and function in that order
GROUND SUBSTANCE • Allows rapid movement • Operates first • Resistance provided by friction between large individual PG molecules and between PGs and collagen fibres • Alterations in molecular structure occur • Ground substance - compressed & displaced into other regions of ligament - depending on direction of force
BLOOD AND BLOOD VESSELS • Blood forced from vessels in ligament to those in alveolar bone marrow • Resistance provided by friction between blood and vessel walls • Again acts as a damper when force applied as blood displaced through vessels through cribriform plate to alveolar bone marrow
PRINCIPLE FIBRE BUNDLES • Only involved after ground substance and other tissue fluids have responded to forces • Fibres become straightened out and absorb axial stress – can increase in number and thickness • Are inelastic – allow no further tooth movement • Prevent direct apposition of cementum and bone surfaces so prevents complete closure of periodontal space
Other changes • Increase in periodontium function :– • 50% increase in PDL thickness • Alveolar bone increases in thickness • Reduction in function :- • PDL narrows, fibre bundles decrease thickness • Alveolar bone decreases in thickness
Occurs during chewing! Forces later than the first occur before teeth have returned to their resting positions Collagen fibres prevent complete closure of periodontal space Proteoglycans become increasingly viscous with increasing rates of loading Teeth move further than after initial force - longer to return to resting position when force removed What happens of we have a second force applied to the tooth after the first force?
Resultant of forces so that tooth moves permanently Socket is remodelled to move with tooth and accommodate new position Tooth eruption Adaptation to jaw growth Physiological mesial drift Orthodontic tooth movement TRANSLOCATORY TOOTH MOVEMENT
Remodelling of PDL = metabolic turnover across whole width of PDL • - FORCE - • PDL fibres breakdown – new ones synthesized • Anchored to cementum and bone by Sharpey’s fibres • New layer of cementum secreted and alveolar socket wall remodelled (resorption and deposition of bone) • Staggered replacement of PDL fibres as • tooth attachment maintained during any movement
Alveolar bone In areas of COMPRESSION, osteoclasts RESORB bone to accommodate tooth movement In areas of TENSION osteoblasts SECRETE bone to fill space left Cementum In areas of TENSION, cementoblasts increase SECRETION of cementum to fill space left In areas of COMPRESSION cementum is RESORBED So what happens to alveolar bone & cementum?
Compression Tension Compression Tension
CLINICAL IMPLICATIONS • Varying structure of alveolar bone means different types of movement needed to extract different teeth – in direction of thinnest bone • Direction of PDL fibres means extraction force is APICALLY directed (push not pull) • Rapid rate of PDL turnover and activity of cementoblasts & osteoblasts means re-attachement of teeth possible • Epithelial rests of Malassez can proliferate = radicular cysts and occasionally more serious pathology