Download
1 / 22
220 likes | 312 Vues
Explore strategies to optimize resource allocation for enteric infections investigations to enhance public health response and outbreak prevention. Examines current challenges and proposed priority recommendations.

E N D
Prioritizing investigations of reported cases of selected enteric infections Richard S. Hopkins, MD, MSPH Leah Eisenstein, MPH CSTE annual meeting, Omaha, NE, June, 2012
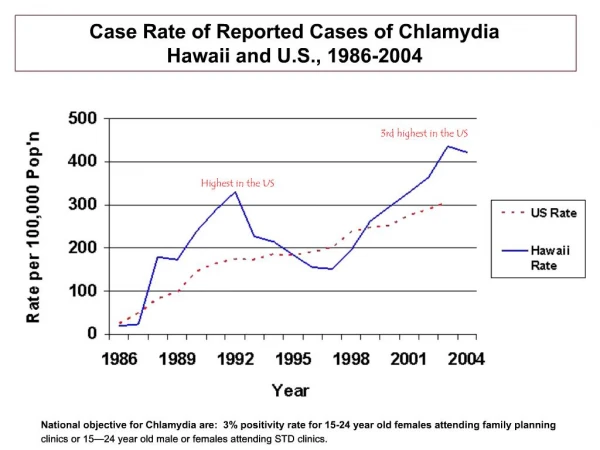
Background • Florida consistently has the highest number, and one of the highest rates, of salmonellosis cases reported among the states • In 2010, there were: • 1211 cases of campylobacteriosis • 408 cases of cryptosporidiosis • 2,139 cases of giardiasis • 6,281 cases of salmonellosis • 1,212 cases of shigellosis • Peak numbers in last ten years: • Campylobacteriosis 1211, cryptosporidiosis 738, giardiasis 2,139, salmonellosis 6,741, shigellosis 2,845 • We serotype fewer than 10% of Salmonella isolates and about 20% of them get a PFGE pattern • This analysis is not about typhoid fever or shigatoxin-producing E. coli
Background • Our standard approach has been that every reported case of each of these infections should be interviewed • Conversations with county health department (CHD) epidemiology staff indicated some lack of clarity as to the purpose of interviews • Epi staff got considerable satisfaction from educating people with cases about how they might have gotten infected and how they could prevent future illnesses in themselves. • CHD staff were spending a lot of time on follow-up testing of cases in sensitive situations to clear them to return
Reality bites • Florida CHDs are getting squeezed financially • By their county commissioners • By the state health department/legislature • By Medicaid • CHD directors are gradually reducing the size of their general epidemiology staffs, and adding duties to those who remain • Florida DOH supports 79 general epidemiology FTEs in CHDs with federal preparedness funds • In some CHDs these are now the majority of epi staff
Rethinking enteric case investigations • In late 2011, the Epidemiology Bureau started a conversation with CHD staff and state-level foodborne investigation staff • Enteric workgroup • Quality improvement workgroup • Started with a high-level principles document • Then some data analysis • Finally a set of priority recommendations for CHD prioritization of enteric investigations • Separately, we are semi-automating the process for creating cases of salmonellosis in Merlin from electronic laboratory reports (J Hamilton presentation)
Preparedness implications • At the same time we were operationalizing the PHEP performance measure about ‘time from receipt of case report to initiation of control measures’ for the six priority PHEP diseases • We had decided to add salmonellosis and shigellosis to the PHEP diseases as we built the capacity to capture the information needed for this performance measure • Whether interviewed • Whether investigated • Whether certain control measures were taken, and when
High-level principles document (August 2011) • Key assumption 1: for these enteric infections, people are most infectious to others while they are ill with diarrhea • To a first approximation, one’s infectiousness to others should be a function of the number of opportunities to soil one’s hands • Some people shed organisms in stool for days to weeks after they recover from their clinical illness, but generally the concentration is lower • Key assumption 2: we don’t know about most of the people with these infections (estimated 2% for salmonellosis)
Purposes of surveillance for these organisms • To detect individual cases in such a way that public health, medical, or behavioral action can prevent spread from the reported case • To detect outbreaks of illnesses due to these agents, early enough to make a difference to the course of the outbreak • To allow a better understanding of the descriptive epidemiology of cases • to be able to focus primary case prevention efforts, and formulate better prevention strategies • To detect outbreaks of illnesses due to these agents • to understand better the events that lead to outbreaks and thus be able to focus outbreak prevention efforts
When can interventions make a difference over one or two incubation periods? • A case is identified while the person is still ill and presumed infectious, and thus interventions may prevent cases • A case is identified after illness has resolved, but while the person was recently infectious and is still potentially infectious. Interventions may still be useful, especially behavior change by infected contacts, and prophylactic treatment of contacts • A common source outbreak is detected early enough that the source of the outbreak can be removed, changing the course of the outbreak • An outbreak that started as a common source outbreak is detected early enough that there is still an opportunity to influence the number of cases spread from person to person
When can investigations make a longer-term difference? • Even if an outbreak is detected after the common source is gone • There is value in learning how the outbreak occurred, so that steps can be taken • to prevent recurrences, and • to help guide public health policy (e.g., in relation to regulation, standards, or inspections)
Key time parameters • Usual duration of illness was taken from CCDM, picking a number toward the upper end of the usual range • From existing Merlin data, we pulled median time intervals by disease for • Case onset to case report to CHD • Diagnosis to case report to CHD • Specimen collection to case report to CHD • Lab report to case report to CHD
Reading the table If a case report of salmonellosis is received 3 days from specimen collection date, the person is likely still ill. If a case report of campylobacteriosis is received 7 days from onset date, the person is likely not still ill.
Our recommended priorities for interview and investigation • Group 1: people whose initial case report indicates they are in a sensitive situation or part of an outbreak. • Group 2: people whose case report is received within the time frames in the table • Group 3: all others • This was conveyed to CHDs March, 2012
Possible drawbacks • Some outbreaks may come to light only as a consequence of interviewing cases reported one by one, and we might miss outbreaks. • This isn’t the most common way we detect outbreaks • If the cases are interviewed late, the outbreak may have come to light anyway, or ended • Some people who are in sensitive situations will be missed if they are in group 2 and are not interviewed, and we will not be able to keep them out and clear them to return. • If their diarrhea has already resolved, the opportunities for prevention in the sensitive setting are less • Most infectious cases are not detected and reported anyway • We will miss opportunities for education and for generating good-will.
Let’s look at some data • Cases reported in CY 2011 • Only confirmed cases • 10,816 cases of 5 diseases • 9,028 interviewed (83%) • From September 1 to December 31, 2011, 18% of interviewed cases were interviewed within recommended timeframe (“timely”) • Range from 10% for salmonellosis to 54% for cryptosporidiosis
Number of confirmed cases > 18 y.o., proportion where interview would have been recommended*, and reduction in interviews, FL, CY 2011 * Based on earliest lab date
Number of confirmed cases < 18 y.o., proportion where interview would have been recommended*, and reduction in interviews, FL, CY 2011 * Based on earliest lab date
Timeliness of interview and diarrhea, for confirmed cases of all five diseases, FL, March 15 – June 1, 2012 Interviewing no-one in Group 3 (late reports) would result in missing about 60% of people with diarrhea at time of interview. The difference in % with diarrhea by timely interview or not is in the wrong direction for giardiasis. We may have underestimated duration of diarrhea in giardiasis. People recovering from giardiasis can have prolonged diarrhea even after the organism is eradicated. 32% of interviews timely is increased from 18% in late 2011
Separating giardiasis from the other four diseases, March 15 - June 1, 2012
Impact on sensitive situations • March 15 – June 2, 2012 • Overall 883 adult cases reported, of whom 703 (80%) interviewed • Food handlers: • 10 interviewed timely, 9 late • 5 symptomatic interviewed timely, 2 late • Healthcare workers • 6 interviewed timely, 17 late • 5 symptomatic interviewed timely, 4 late • Child care workers • 4 interviewed timely, 5 late • 2 symptomatic interviewed timely, 5 late • Among 980 cases in children under age 18, for children in child care: • 70 interviewed early, 118 late • 23 symptomatic interviewed timely, 38 late
What are CHDs doing with our recommended priorities? • Survey of CHDs in late April: 29 out of 40 CHDs were adopting the prioritization • Many said they would use the priority list to do only very brief interviews with those in Group 3 • % reported as interviewed down from 84% Sept – Dec 2011 (before recommendations made) to 82% March 15 – June 1, 2012. • % of interviews that are timely has gone up from 18% to 32% • % of people symptomatic at time of interview has gone up from 37% to 42%
Costs and benefits • Following this approach could reduce annual number of interviews completed by over 5000 • We would not interview over half of the people who still had diarrhea at the time of interview • We would not identify about half of the adults in sensitive situations who still had diarrhea at time of interview • We would not identify 38% of children in child care who still had diarrhea at time of interview • CHDs are being more selective about whom they interview (more are timely, more are symptomatic)