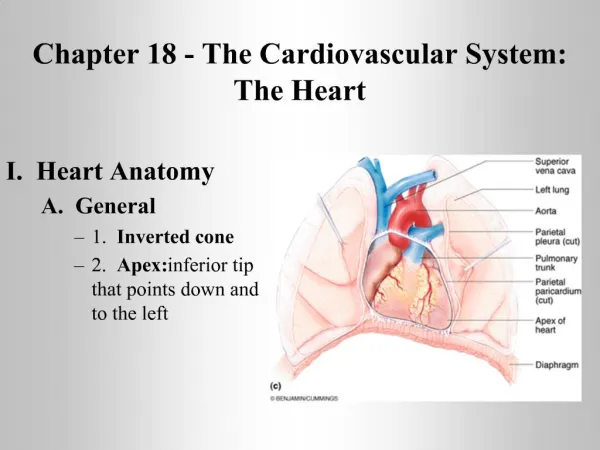
Chapter 18 --The Heart
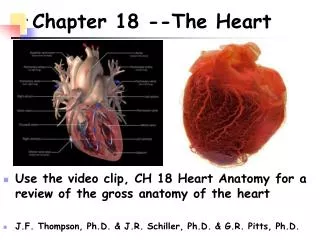
Chapter 18 --The Heart. Use the video clip, CH 18 Heart Anatomy for a review of the gross anatomy of the heart J.F. Thompson, Ph.D. & J.R. Schiller, Ph.D. & G.R. Pitts, Ph.D. Pericardium. The sac containing the heart. 3 Layers Form the Heart’s Wall -. Epicardium (outer) Myocardium (middle)

Chapter 18 --The Heart
E N D
Presentation Transcript
Chapter 18 --The Heart • Use the video clip, CH 18 Heart Anatomy for a review of the gross anatomy of the heart • J.F. Thompson, Ph.D. & J.R. Schiller, Ph.D. & G.R. Pitts, Ph.D.
Pericardium The sac containing the heart
3 Layers Form the Heart’s Wall - • Epicardium (outer) • Myocardium (middle) • Endocardium (inner)
inflammation of the pericardium painful may damage the lining tissues may damage myocardium Pericarditis fibrinous pericarditis
Cardiac Tamponade • a buildup of pericardial fluid, or • bleeding into the pericardial cavity • may result in cardiac failure • Elizabeth, Empress of Austria (d. 1898) by assassination with a hat pin
Chambers of the Heart • Internally - 4 compartments • R/L atria with auricles • R/L ventricles • Interatrial septum separates atria • Interventricular septum separates ventricles • Left ventricular wall is much thicker because it must pump blood throughout the body and against gravity LA RA LV RV
Blood Flow through the Heart • Right atrium (RA) - receives deoxygenated blood from three sources • superior vena cava (SVC) • inferior vena cava (IVC) • coronary sinus (CS) SVC (CS RA IVC
Blood Flow through the Heart • Right ventricle (RV) • receives blood from RA • pumps to lungs via Pulmonary Trunk (PT) • Pulmonary Trunk (PT) - from RV branches into the pulmonary arteries (PA) • Pulmonary arteries • deoxygenated blood from the heart to the lungs for gas exchange • right and left branches for each lung • blood gives up CO2 and picks up O2 in the lungs • Pulmonary veins (PV) - oxygenated blood from the lungs to the heart PA PA PT RA RV
Blood Flow through the Heart • Left atria • receives blood from PV • pumps to left ventricle • Left ventricle (LV) • sends oxygenated blood to the body via the ascending aorta • aortic arch • curls over heart • three branches off of it feed superior portion of body • thoracic aorta • abdominal aorta Aortic arch LA PV PV LV
Schematic of Circulation Know the names of the valves indicated here.
Schematic of Circulation Review Routes
Myocardial Blood Supply • Myocardium has its own blood supply • coronary vessels • simple diffusion of nutrients and O2 into the myocardium is impossible due to its thickness • Collateral circulation = duplication of supply routes and anastomoses (crosslinked connections) • Heart can survive on 10-15% of normal arterial blood flow
Myocardial Blood Supply • Arteries • first branches off the aorta • blood moves more easily into the myocardium when it is relaxed between beats during diastole • blood enters coronary capillary beds [note the collateral circulation]
Myocardial Blood Supply • Coronary veins • deoxygenated bloodfrom cardiac muscle is collected in the coronary veins and then drains into the coronary sinus • deoxygenated blood is returned to the right atrium
Coronary Circulation Pathologies • Compromised coronary circulation due to: • emboli: blood clots, air, amniotic fluid, tumor fragments • fatty atherosclerotic plaques • smooth muscle spasms in coronary arteries • Problems • ischemia (decreased blood supply) • hypoxia (low supply of O2) • infarct (cell death)
Pathologies (cont.) • Angina pectoris - classic chest pain • pain is due to myocardial ischemia – oxygen starvation of the tissues • tight/squeezing sensation in chest • labored breathing, weakness, dizziness, perspiration, foreboding • often during exertion - climbing stairs, etc. • pain may be referred to arms, back, abdomen, even neck or teeth • silent myocardial ischemia can exist
Pathologies (cont.) • Myocardial infarction (MI) - heart attack • thrombus/embolus in coronary artery • some or all tissue distal to the blockage dies • if pt. survives, muscle is replaced by scar tissue • Long term results • size of infarct, position • pumping efficiency? • conduction efficiency, heart rhythm
Pathologies (cont.) • Treatments • clot-dissolving agents • angioplasty (bypass surgery) • Reperfusion damage • re-establishing blood flow may damage tissue • oxygen free radicals - electrically charged oxygen atoms with an unpaired electron • radicals indiscriminately attack molecules: proteins (enzymes), neurotransmitters, nucleic acids, plasma membrane molecules • further damage to previously undamaged tissue or to the already damaged tissue
Valve Structure • Dense connective tissue covered by endocardium • AV valves • chordae tendineae - thin fibrous cords • connect valves to papillary muscles
Valve Function • Opening and closing a passive process • when pressure low, valves open, flow occurs • with contraction, pressure increases • papillary muscles contract pull valves together
Valves of the Heart • Function to prevent backflow of blood into/through heart • Open and close in response to changes in pressure in heart • Four key valves: tri- and bi-cuspid (mitral) valves between the atria and ventricles and semi-lunar valves between ventricles and main arteries • Valves also close the entry points to the atria Tricuspid Bicuspid (Mitral) Semi-lunar
Atrioventricular (AV) valves • Separate the atria from the ventricles • bicuspid (mitral) valve – left side • tricuspid valve – right side • note the feathery edges to the cusps anterior bicuspid tricuspid
Semilunar valves • in the arteries that exit the heart to prevent back flow of blood to the ventricles • pulmonary semilunar valves • aortic semilunar valves • Pathologies • Incompetent – does not close correctly • Stenosis – hardened, even calcified, and does not open correctly
Normal Action Potential Review in Chapter 11
Cardiac Muscle Action Potential • Contractile cells • near instantaneous depolarization is necessary for efficient pumping • much longer refractory period ensures no summation or tetany under normal circumstances
Cardiac Muscle Action Potential electrochemical events
Cardiac Muscle Action Potential sarcolemma’s ion permeabilities • opening fast Na+ channels initiates depolarization near instantaneously • opening CA++ channels while closing K+ channels sustains depolarization and contributes to sustaining the refractory period • closing Na+ and Ca++ channels while opening K+ channels restores the resting state repolarization
Cardiac Muscle Action Potential • long absolute refractory period permits forceful contraction followed by adequate time for relaxation and refilling of the chambers • inhibits summation and tetany
Pacemaker Potentials • leaky membranes • spontaneously depolarize • creates autorhythmicity • the fact that the membrane is more permeable to K+ and Ca++ ions helps explain why concentration changes in those ions affect cardiac rhythm
Conduction System and Pacemakers • Autorhythmic cells • cardiac cells repeatedly fire spontaneous action potentials • Autorhythmic cells: the conduction system • pacemakers • SA node • origin of cardiac excitation • fires 60-100/min • AV node • conduction system • AV bundle (Bundle of His) • R and L bundle branches • Purkinje fibers It’s as if the heart had only two motor units: the atria and the ventricles!
Conduction System and Pacemakers • Arrhythmias • irregular rhythms: slow (brady-) & fast (tachycardia) • abnormal atrial and ventricular contractions • Fibrillation • rapid, fluttering, out of phase contractions – no pumping • heart resembles a squirming bag of worms • Ectopic pacemakers (ectopic focus) • abnormal pacemaker controlling the heart • SA node damage, caffeine, nicotine, electrolyte imbalances, hypoxia, toxic reactions to drugs, etc. • Heart block • AV node damage - severity determines outcome • may slow conduction or block it
Conduction System and Pacemakers • SA node damage (e.g., from an MI) • AV node can run things (40-50 beats/min) • if the AV node is out, the AV bundle, bundle branch and conduction fibers fire at 20-40 beats/min • Artificial pacemakers - can be activity dependent
Atrial,Ventricular Excitation Timing • Sinoatrial node to Atrioventricular node • about 0.05 sec from SA to AV, 0.1 sec to get through AV node – conduction slows • allows atria time to finish contraction and to better fill the ventricles • once action potentials reach the AV bundle, conduction is rapid to rest of ventricles
Extrinsic Control of Heart Rate • basic rhythm of the heart is set by the internal pacemaker system • central control from the medulla is routed via the ANS to the pacemakers and myocardium • sympathetic input - norepinephrine • parasympathetic input – acetylcholine
Electrocardiogram • measures the sum of all electro-chemical activity in the myocardium at any moment • P wave • QRS complex • T wave
Cardiac Cycle • Relationship between electrical and mechanical events • Systole • Diastole • Isovolumetric contraction • Ventricular ejection • Isovolumetric relaxation
Cardiac Output • Amount of blood pumped by each ventricle in 1 minute • Cardiac Output (CO) = Heart Rate x Stroke Volume • HR = 70 beats/min • SV = 70 ml/beat • CO = 4.9 L/min * *Average adult total body blood volume = 4-6 L
Cardiac Reserve • Cardiac Output is variable • Cardiac Reserve = maximal output (CO) – resting output (CO) • average individuals have a cardiac reserve of 4X or 5X CO • trained athletes may have a cardiac reserve of 7X CO • heart rate does not increase to the same degree
Regulation of Stroke Volume • SV = EDV – ESV • EDV • End Diastolic Volume • Volume of blood in the heart after it fills • 120 ml • ESV • End Systolic Volume • Volume of blood in the heart after contraction • 50 ml • Each beat ejects about 60% of the blood in the ventricle
Most important factors in regulating SV: preload, contractility and afterload Preload – the degree of stretching of cardiac muscle cells before contraction Contractility – increase in contractile strength separate from stretch and EDV Afterload – pressure that must be overcome for ventricles to eject blood from heart Regulation of Stroke Volume
Preload • Muscle mechanics • Length-Tension relationship? • fiber length determines number of cross bridges • cross bridge number determines force • increasing/decreasing fiber length increases/decreases force generation • Cardiac muscle • How is fiber length determined/regulated? • Fiber length is determined by filling of heart – EDV • Factors that effect EDV (anything that effects blood return to the heart) increases/decreases filling • Increases/decreases SV
Preload • Preload – Frank-Starling Law of the Heart • Length tension relationship of heart • Length = EDV • Tension = SV As the ventricles become overfilled, the heart becomes inefficient and stroke volume declines. “cardiac reserve”
Contractility • Increase in contractile strength separate from stretch and EDV • Do not change fiber length but increase contraction force? • What determines force? • How can we change this if we don’t change length?
Sympathetic Stimulation • Increases the number of cross bridges by increasing amount of Ca++ inside the cell • Sympathetic nervous stimulation (NE) opens channels to allow Ca++ to enter the cell
Positive Inotropic Effect • increase the force of contraction without changing the length of the cardiac muscle cells
Afterload • if blood pressure is high, it is difficult for the heart to eject blood • more blood remains in the chambers after each beat • heart has to work harder to eject blood, because of the increase in the length/tension of the cardiac muscle cells
Regulation of Heart Rate • Intrinsic • Pacemakers • Bainbridge effect • Increase in EDV increases HR • Filling the atria stretches the SA node increasing depolarization and HR