PNEUMONIA
PNEUMONIA. Diagnosis Definition & Explanation of Diagnosis Etiology & Risk Factors Incidences Among Gender, Age, & Ethnicity Prognosis Signs & Symptoms. By: Marjorie Johnson. definition. Pneumonia : inflammation of the respiratory bronchioles and alveoli

PNEUMONIA
E N D
Presentation Transcript
PNEUMONIA Diagnosis Definition & Explanation of Diagnosis Etiology & Risk Factors Incidences Among Gender, Age, & Ethnicity Prognosis Signs & Symptoms By:Marjorie Johnson
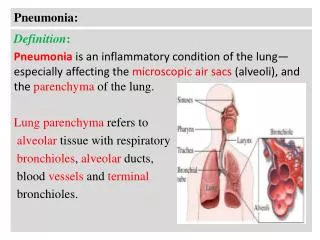
definition Pneumonia: inflammation of the respiratory bronchioles and alveoli Either infectious or non-infectious Infectious: bacteria, viruses, fungi, protozoa and other microbes Non-infectious: aspiration of gastric contents and inhalation of toxic or irritating gases
DIAGNOSIS Pneumonia is often diagnosed with difficult breathing because the airway is filled with mucus and fluid A person with pneumonia often produces delicate crackling noises or wheezing in the area of the lung affected by pneumonia In a lung with pneumonia, the sound can be dull or muffled because the air sacs are filled with fluid instead of air A doctor may take a chest x-ray to confirm a diagnosis of pneumonia
Other risk factors People with problems with heart, liver, or kidneys. Patient with HIV/AIDS whose immune system are very weak. Patient who taking medication that weaken the immune system such as cancer patients. Patients that smoke, abuse alcohol. Exposure to certain chemicals, past surgery Patients hospitalized in an intensive care of certain disease (ex: coma)
prognosis More than a million people are hospitalized each year for pneumonia 1 in 4 people who had pneumonia died Community-acquired pneumonia is responsible for 350,000 to 620,000 hospitalizations Older adults have lower survival rates than younger people Pneumonia kills between 40,000 to 70,000 people each year
Signs & Symptoms Most people who develop pneumonia initially have symptoms of a cold which are followed by: High fever Shaking Chills Sharp chest pain Tachycardia Tachypnea Cough with sputum production
PNEUMONIA Diagnostic tests (include rationale & nursing implications Medical Treatment and Nursing Implications Surgical Treatment and Nursing Implications Prevention Complications Discharge/Client teaching By:Stacy Moyston-Duckie
DIAGNOSTIC TESTS • Diagnostic tests are usually done by a medical doctor who would examine the client by auscultations of the lungs for evidence of delicate crackling noises or wheezing in the area that is infected. In a lung with pneumonia, the sound can be dull or muffled because the air sacs are filled with fluid instead of air. • Based on these findings the doctor will order certain test to be done to identify the organism that is responsible for this illness.
DIAGNOSTIC TESTS • sputum gram stain and culture and sensitivity, complete blood count (CBC) with white blood cell (WBC), arterial blood gases, pulse oximetry, chest x-ray and fiberoptic bronchoscopy • These tests may show the type of organism (bacterial, viral or fungal) causing pneumonia, also other conditions such as heart failure, lung cancer, or acute bronchitis.
Medical treatment With medical treatment the patient with pneumonia is generally treated with: • Immunization: Pneumococcal vaccine is recommended for people over age 65, for immunocompromised people, and for those with chronic cardiac or respiratory conditions, diabetes mellitus, alcoholism, or other chronic disease. • Medications: Medications used to treat pneumonia may include antibiotics to eradicate causative organisms and bronchodilators to reduce bronchospam and improve ventilation. • Oxygen therapy: Oxygen may be ordered when pneumonia interferes with gas exchange. The nasal cannula delivers 24% to 45% oxygen (room air is 21% oxygen) with flow rates of 2 to 6 liters per minute. • Other therapies: Increasing fluid intake to 2,500 to 3,000 mL/day helps liquefy secretions, making them easier to cough up and expectorate. • Another effective method is percussion, which is done by rhythmically striking or clapping the chest wall with cupped hands. Cupping traps air between the palm and the skin, causing vibrations that loosen respiratory secretions. Postural drainage uses gravity to help remove secretions from a particular lung segment.
SURGICAL TREATMENT • Thoracotomy is the standard surgery for pneumonia. • It requires general anesthesia and an incision to open the chest and view the lungs. The surgeon most times has to remove dead or damaged lung tissue. In extreme cases the entire lobe of the lung is removed.
Treatment and nursing implications • Clients being treated for pneumonia need therapeutic care in order to successfully recover. The priority of nursing care for clients with pneumonia is its effects on the client’s ability to maintain open airways and on the exchange of gases in the alveoli. • The nurse must always wash his/her hands and wear gloves, if indicated. Hand washing and gloves help to prevent the spread of infection. • If the person has difficulty breathing, he or she is given oxygen, usually by mask or cannula. Adjust the client’s position. • An orthopneic position may be necessary. Proper positioning helps the person to be more comfortable and to breathe more easily. Place a pillow lengthwise under the back. This action encourages fuller chest expansion. • Assess the client’s vital signs at least every 4 hours. Frequent monitoring is necessary to allow for prompt detection and early intervention if problems arise.
PREVENTION • There are a number of steps a person can take to help prevent getting pneumonia. • Stop Smoking!!!Smoking puts a smoker at high risk in getting pneumonia. • One must avoid contact with people who suffer from respiratory tract infections, such as colds and influenza (flu), measles and chickenpox. • Pneumonia may develop or put the client at risk for developing these types of infections. Vaccination is given mostly to adults over 65 years of age who are at greater risk of developing pneumonia as well as for younger people who are chronically ill.
PREVENTION • Also daily diets should include foods such as fresh, dark-colored fruits and vegetables, which are rich in antioxidants and other important food chemicals that help, boost the immune system. • Children are given vaccination against certain diseases such as measles, and chickenpox. Mineral zinc may also reduce the risk of pneumonia in children. Zinc can be found in foods that we eat such as, seafood, lean red meats, beans, and cereals.
complications • Clients with pneumonia must be treated immediately to avoid serious complications such as by way of entering in the bloodstream or by cross- contamination to other parts of the body. • Without proper treatment, pneumonia can lead to such life-threatening complications as septic shock, hypoxemia, and respiratory failure. The infection can also spread within the patient’s lungs, causing empyema or lung abscess.
Discharge/client teaching • It is very important that the nurse educate the client about the disease and how to do self-care. • The nurse must explain all procedures (especially intubation and suctioning) to the patient and his family. Emphasize the importance of adequate rest to promote full recovery and prevent a relapse. • Stress the need to take the entire course of medication, even if he feels better, to prevent a relapse. • Teach the patient procedures to clear lung secretions, such as deep-breathing and coughing exercises, as well as home oxygen therapy. Explain deep breathing and pursue-lip breathing.
Congestive heart failure Yvonne Prempeh Medical Surgical Nursing 1 July 23, 2007
Objectives • Definition and explanation of congestive heart failure • Epidemiology: incidences among gender, age and ethnicity • Etiology and risk factors • Diagnosis of CHF
Definition and explanation of CHF • structural or functional cardiac disorder impairing the filling and pumping ability of the heart • highly specialized muscular organ • normal heart pump 50% of total blood • failing heart pumps </= 40% of total blood
Epidemiology • Younger men are more likely than women to develop myocardial infarction • People >/= 65 years have higher risks for CHF • 48,500 heart attacks are associated with CHF • 23,500 heart attacks occur in women
Epidemiology cont’d • Asians and Latinos tend to suffer least cases of cardiovascular diseases • African Americans are at a higher risk for developing severe CHF • recurrent hospitalization rate • increased mortality rate due to severe CHF ( www.american heart.org; National Institutes of Health)
Etiology and risk factors • Causes of CHF: • myocardial ischemia • hypertension • various types of arrhythmias • anemia • hyperthyroidism • hypothyroidism • diabetes mellitus • endocarditis • myocarditis • congenital heart defects • artherosclerosis • cardiomyopathy
Etiology and risk factor cont’d • increased cholesterol intake • increased intake of fats • increased sodium intake • lack of exercise • morbid obesity • diabetes mellitus • hypertension
Diagnosis of CHF • Targeted history and physical exam • Tests: • BNP ( B-type Natriuretic Peptide) • normally secreted in ventricles during filling and stretching • BNP < 100 pg/ml : No CHF • BNP between 100-300 pg/ml: suggestive CHF • BNP > 600 pg/ml: moderate CHF • BNP > 900pg/ml: severe CHF (www.clevelandclinic.org/heart center)
Diagnosis cont’d • Tests cont’d: • Serial EKG’s and cardiac iso-enzymes q6h x 3 • Troponin I • CK (creatine kinase) • CKMB (specific from heart muscle fraction) • CKMB Index (calculated by lab) • CBC • Chest x-ray: to detect pulmonary edemas a result of edema • Two dimensional echocardiogram: to check the pumping ability of the heart and the function of the heart • Stress test to evaluate for myocardial ischemia
Signs and Symptoms Main manifestations to watch out for: Fatigue and dyspnea ( difficulty breathing) = Due to excess fluid in the body and fluid in the lungs that causes congestion. = Mostly observable when a person is walking halfway and gets tired easily eventhough he just walk halfway. Edema or swelling of the ankle and feet) = Due to fluid overload in the tissue which causes congestion. = mainly observe during the day and every time the feet is used. Other symptoms include: Nausea, abdominal pain and decreased appetite.
Diagnostic Tests Tests to confirmed the presence of congestive heart failure: EKG or EGC ( Electrocardiogram) 2. X-ray examination 3. Echocardiography 4. Cardiac catherization Purpose: Evaluate heart function and valve dysfunction. NURSING IMPLICATION: Discuss situation with the client the procedure. Distinguish the possible effects of the procedure to the well-being of the patient. Rationale: Discussing will help the client to be more familiar with the procedure hence, it will decrease anxiety. Client will be able to deal with her fear by the information gathered from the nurse.
Medical Treatment Digoxin = Cardioglycoside = slows heart rate. = stimulate heart muscle which increases the force of systole. =Decreased the workload of the heart. NURSING IMPLICATION: = Monitor apical pulse before administering the medication. = If less than 60 bpm, withhold the medication, then notify MD. Diuretics =Help fluid from building up =Decrease fluid retention = make the fluids run through the kidneys NURSING IMPLICATION: Monitor BP, I&O, daily weight. Assess feet, legs, and sacral area for edema DAILY>
Prognosis Congestive heart failure has a very poor prognosis. Only 50% of CHF patients lives within 5 years. On the other hand, only 20% survive within 8 to 12 years prior to diagnose. HALF OF THE PATIENT WILL DIE IN 5 years.
Congestive heart failure Surgical Treatment/ Nursing Implications Prevention Complications Discharge/Client Teaching by Marie Jimenez
Surgical Treatment Types of surgical treatment for CHF: Cardiac transplantation Dynamic cardiomyoplasty
Cardiac Transplantation Primary treatment for end-stage heart failure Transplanted organs are from young accident victims with no evidence of cardiac trauma Client or (recipient) heart is removed, leaving posterior atria intact Donor heart is sutured to the remaining atrial walls
Cardiac Transplant: NURSING IMPLICATIONS Risks for surgical treatment of CHF: Infection Rejection of donor’s heart Nursing Implication: Monitor for infection Administering immunosuppresive drugs to prevent the rejection of the transplanted organ Route: IV, PO, IM
Dynamic cardiomyoplasty Dynamic cardiomyoplasty involves using the client’s own skeletal muscle (particularly the latissimus dorsi) to enhance the function of the heart and improve circulation. The muscle is positioned around the heart or aorta, and a cardiomyostimulator and leads are implanted to stimulate muscle contractions. This type of surgical procedure may be implemented as an alternative to cardiac transplantation for clients who refuse organ transplantation.
PREVENTION The prevention of CHF includes modifiable lifestyle changes relating to diet, smoking, alcohol, and exercise Limit sodium intake Alcoholics Anonymous & Smoking cessation programs Providing awareness of the negative effects of smoking and alcohol and recommending “regular, moderate exercise to improve their overall fitness” will greatly reduce in the prevention of congestive heart failure. (Merck Manual, 1997)
complications Hepatomegaly (enlargment of the liver) Spenomegaly (enlargement of the spleen) Thrombus & emboli Cardiogenic shock which “occurs when the left ventricle is unable to supply the tissues with enough oxygen and nutrients to meet their needs. [It] is a life-threatening condition that requires immediate treatment (Williams, 2003, p. 332) Picture on right: IABP (intra-aortic balloon pump) to increase coronary perfusion
Discharge & client teaching Nursing interventions for discharge: Explain heart failure and its effects on the client’s life – this helps the client understand the reasons for ordered treatments Stress the importance of medications in managing heart failure and provide verbal and written information regarding each specific medication to encourage compliance Teach the client and family about the prescribed diet Instruct to keep regular follow-up appointments to monitor disease progression and effects of therapy
Chronic Obstructive Pulmonary Disease(COPD) Student Name: Na Pang
Nursing Diagnosis: • Ineffective Airway Clearance • Imbalanced nutrition: less than body requirements, • compromised family copying • Decisional conflict: smoking.
Definition and Explanation of Diagnosis: • Chronic obstructive pulmonary disease (COPD) is a term referring to two lung diseases, chronic bronchitis and emphysema, that are characterized by obstruction to airflow that interferes with normal breathing. Both of these conditions frequently co-exist, hence physicians prefer the term COPD.
Etiology and Risk Factors: • Etiology: In COPD, there is decreased elastic recoil of the lungs (mainly emphysema) and increased airway resistance (mainly bronchitis). • Risk factors: Smoking is the primary risk factor for COPD. Approximately 80 to 90 percent of COPD deaths are caused by smoking.
Incidence Among Gender, Age and Ethnicity: • 1. Chronic bronchitis affects people of all ages, but is higher in those over 45 years old. • 2. Females are more than twice as likely to be diagnosed with chronic bronchitis as males. In 2004, 2.8 million males had a diagnosis of chronic bronchitis compared to 6.3 million females. • 3. Chronic bronchitis prevalence for Hispanics (27.7 per 1,000) was significantly lower than for both Whites (45.7 per 1,000) and Blacks
COPD PROGNOSIS • None of the existing medications for COPD has been shown to modify the long-term decline in lung function that is the hallmark of this disease. Therefore, the goal of pharmacotherapy for COPD is to provide relief of symptoms and prevent complications and/or progression of the disease with a minimum of side effects.
Signs and symptoms: • 1. Cough • 2. Sputum (mucus) production • 3. Shortness of breath, especially with exercise • 4. Wheezing (a whistling or squeaky sound when you breathe) • 5. Chest tightness
Chronic Obstructive Pulmonary Disease Student Practical Nurse, Anaïse Ikama Spring II 2007
Diagnostic TestsThe following test can be used to diagnose COPD • Pulmonary function testing a spirometry is used to identifies how much air your lung can hold and how fast you can blow the air out of your lung • Chest X-ray helps in the identification of emphysema (causes large abnormal air spaces in the lungs by destroying alveolar walls)
Diagnostic Test • Serum alpha1-antitrypsin levels to screen the enzyme deficiency that can cause lung tissue destruction • Arterial Blood Gas measures deficiency of oxygen • Other test such as a computed Tomography can determine if the client will benefit from surgery
Medical Treatment • Bronchodilators as prescribed to relax the muscles that wrap around the airways allow tubes to become larger and easier to breath through • Inhaled steroids/corticosteroids reduces swelling in the breathing tube