Download
1 / 36
420 likes | 1.56k Vues
VENTRICULAR SEPTAL DEFECT (VSD). It is a hole on interventricular septum Congenital or acquired. VENTRİKÜLER SEPTAL DEFEKT (VSD). Congenital. Acquired. It is mostly seen as a complication of acute myocardial infaction . Rarely trauma is a cause.

E N D
VENTRICULAR SEPTAL DEFECT (VSD) It is a hole on interventricularseptumCongenitaloracquired
VENTRİKÜLER SEPTAL DEFEKT (VSD) Congenital Acquired It is mostlyseen as a complication of acutemyocardialinfaction. Rarelytrauma is a cause . • Isolated VSD can be seen in nearly2per1000 livebirths. • It is themostfrequentcongenitalcardiacanomaly. • can be associatedwithotheranomalies.
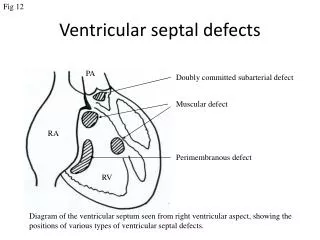
VSD MORPHOLOGICAL CLASSIFICATION Yerleşim Neighbourhood Tricuspidvalve , conductionsystem(posteroinferior) Bothsemilunarvalves ( Rightcoronarycusp) It is surroundedbymuscle Conductionsystem(posteriorinferior) Perimembraneous %80 Subarterial %5-10 ( Juxta- arterial, conal, infundibular) Muscular %5 Inletseptal <%5 (AV kanal , AV septal)
CLASS ACCORDING TO SIZE • VSD büyüklükleri; aort orifis çapına göre değerlendirilebildiği gibi • VSD rezistans indekslerine (Rİ) göre de değerlendirilebilir. • VSD Rİ = LVP - RVP x m2 • Qp-Qs • LVP= Sol ventrikül basıncı; • RVP= Sağ ventrikül basıncı; • Qp= Pulmoner kan akımı; • Qs= Sistemik kan akımı; • m2= Vücut alanı
VSD LargeVSD ModerateVSD VSD diameter < Aort diameter RVP=1/2 LVP Qp/Qs≥2 • VSD diameter≥ Aorticdiameter • VSD Rİ < 20 Ü/m2 • Resistancetoflow is small • RVP = LVP • Qp/Qsratiodepends on degree of pulmonaryvascularresistance(PVR).
VSD SmallVSD • VSD has not enoughspacetoincreasetherightventricularsistolicpressure. • VSD Rİ>20Ü/m² • Qp/Qs<1.75
Symptomsandsigns • Patientswithlarge VSD andincreasedQp/Qs • Weakperipheralpulses • Tachypnea, subcostaldrawings, profusesweating • Hepatomegaly, highjugularvenouspressure, • Difficulty in feeding, growthretardation
Large VSD andlight PVR • There is a strongpansystolic (holosystolic) murmurorthrill on theleftparasternalregionoverthe 3th ,4th intercostalspace ( subarterial VSD on 2nd, 3th ICS), • Apicaldiastolicmurmurbecause of increasedbloodflowpassingthroughoutth mitral valve. • S2 isstrongandsplittedduetoincreasedpulmonaryflow.
Large VSD andhigh PVR • Lefttorightshuntdecreasesandbecomesbidirectional. • Hyperactivity of theheartandcardiomegalydecrease. • Pansytolicmurmurchange in character, becomesshortandsoft. • Apicaldiastolicmurmur is no moreheard. • S2 is forcefull. • ThepatientbecomescyanoticIf PVR>SVR. (Eisenmengersendrome)
CHEST X-RAY Large VSD andlight PVR Large VSD andhigh PVR
PatientswithModerate size VSD • Pansystolicmurmur • Light – moderateleftandrightventricularenlargement.
small VSD • There is harshpansystolicmurmurduetosmall VSD andshunt. • EKG ve Chest X ray are normal.
Echocardiography: • 2 Dimensional, colourDoppler ECHO • Give us incredibleinformationaboutthesituationand size of the VSD • QP/QS can be calculated. • AssociatedanomalieslikeAorticcoarctationand PDA .
HEART CATHETERIZATION • TomeasurePulmonaryarterypressure, • LefttorightshuntandPVR • To define theplace, numberand size of the VSD • Toshowdefinitelytheassociatiedanomalies.
SPONTANOUS CLOSURE • Large VSD ; • 1 month %80 • 3 month %60 • 6 month %50 • 12 month %25 spontaneousclosurechance.
SPONTANOUS CLOSURE Lesschancetoclose Morechancetoclose Juxta-tricuspid Muscular (outlet) • Perimembranous • Juxtaaortic • Inletseptal
COMPLICATIONS • PulmonaryVasculardisease • Large VSD can haveseriouspulmonaryresistance (Rp) in first 2 years of life
PulmonaryVasculardisease (HeathEdwardsClassification) • Grade 1: Medialhyperthrophy. • Grade 2: Medialhyperthrophyandintimalcellularproliferation • ---------------------------------------------------------------------- • Grade 3: Medialhyperthrophyandintimalfibrosisearlygeneralizedvasculardilatation • Grade 4: Generalizedvasculardilatation, vascularoclusionsduetointimalfibrosis, plexiformlesions. • Grade 5: Cavernous ve angiomatoidlesions. • Grade 6: Necrotizingarteritis.
InfectiveEndocarditis • It is seen 0.15-0.3% of patientperyear • MoreoftensmallandmoderateVSDs • Rightsidedvegetations (Tricuspid kapak) • Lunginfections • Aorticinsufficiency • Inthefirstdecade 35-80 % . • Especiallysubarterial VSD
EarlyDeath • 9 % of thepatientwithlarge VSD diewithinthe 1st year. • PDA, Coarctation, large ASD • Recurrentlunginfections (Viral). • Pulmonaryedema (heartfailure). • AfterthefirstdecadeEisenmengercomplications (Hemoptisis, polycytemia, cerebralemboli, abscesses, rightheartfailure) • 50% of patientsdiebefore 35 years of age.
PulmonaryVascularResistance • Resistance • < 4 ünite m2 Normal • < 5 ünite m2mildlyelevated • < 8 ünite m2moderatelyelevated • > 8 ünite m2severelyelevated
INDICATIONS FOR OPERATION • Large VSD • Everypatientwithintractableheartfailureundermedicaltreatment can be operatedbefore 12 months. • (Swisscheese – Pulmonarybanding) • Ifthere is growthfailureorRp >8ü m2 at 6 month, theoperationshould be performed.( IfRp < 4ü m2 , theoperation can be deferreduntill 12 month.) • AfterinfancyRp is truelyandpreciselymeasured. IfRp < 8ü m2 patient can be operated, IfRp >8ü m2 , afterisoproteronolperfusionremeasurementshould be madeIfRp ≤ 7ü m2patient can be operated,
INDICATIONS FOR OPERATION • Moderate VSD • IfPpa 40-50 mmHgandQp/Qs is about 3 Rp is rarelyelevatesandwe can waitforoperationuntill5 years of age. • Small VSD • İnfectiveendocarditis, ventriküldysfunction is rarelyseen (After 10 years of age)
SURGICAL TREATMENT • Pulmonarybanding • 1-Swisscheeseseptumwithintractableheartfailure • Complications • Hospitalmortality is high • Pulmonarystenosis, migration
PATCH CLOSURE • Perikardial, Dacronand PTFE patches can be usedforclosure. • Interruptedsuture (Teflon pledgetedsingle) orcontinuoussuture can be used. • Fromtherightatrium------ Perimembranous. • Fromtherightventricle----- subarterial • (Ventricularscar can cause RBBB, Arythmia yüksek)